Adolescence is a significant period of human growth and maturation; unique changes occur and many adult patterns are established during this period. In addition, the proximity of adolescence to biological maturity and adulthood may provide final opportunities for preventing adult health problems. Human growth and maturation are continuous processes, and transitions from childhood into adulthood are not abrupt. In contrast with the previous age groups, which are defined by chronologic age, adolescence begins with pubescence, the earliest signs of development of secondary sexual characteristics, and continues until morphologic and physiologic changes approximate adult status, usually near the end of the second decade of life.
Whereas adolescence is clearly an important period in human development, it has often failed to receive the attention given to earlier periods in childhood with regard to health-related uses and interpretations of anthropometry. Historically, the rapid changes in somatic growth in adolescence, the problems of dealing with variation in maturation, and the difficulties involved in separating normal variations from those associated with health risks have all discouraged researchers from developing a body of knowledge about adolescent anthropometry that would link it directly to health determinants and outcomes.
Adolescent is defined by WHO as a person between 10-19 years of age. There are about 1.2 billion adolescents worldwide and one in every five people in the world is an adolescent. Adolescents constitute 18-25% of the population in member countries of South East Asia Region (World Health Organization, 2011 June).
Adolescence is a phase of rapid growth and development during which physical, sexual and emotional changes occur. Adolescents are not homogeneous group and their needs vary with their gender, stage of development, life circumstances and the socio economic conditions in which they live. Although adolescents are generally considered to be healthy yet many of them die prematurely due to accidents, suicide violence, pregnancy related complications and other preventive or treatable illnesses.
Age group
According to WHO definitions, young people are aged 10 to 24 years*. Adolescents are a large and growing segment of the global population. The largest share of adolescents is and will continue to be in Asia, which is home to 60 % of the world’s population (UNFPA, 1998). However, in assessing commitments made since the International Conference on Population and Development (ICPD) in 1994, adolescent’s sexual and reproductive health rights remain inadequately addressed. While adolescence generally is a healthy period of life, many adolescents are less informed, less experienced, and less comfortable accessing family planning and reproductive health services than adults. Adolescents circumstances and needs vary tremendously depending on social and individual characteristics such as age, sexual activity, schooling and employment status as well as their position within the range of adolescent years. It is important to recognize that while the world in many cultures expands for boys, giving them greater autonomy, mobility, opportunity and power, many girls are systematically being deprived of these advantages (UNFPA 2000).
Adolescent girls in Bangladesh
Adolescents (10 to 19 years) make up around 21 per cent of the population of Bangladesh. Typically, adolescence is not recognized as a transitional, formative phase of life, but rather is considered as a dramatic shift from childhood to adulthood that takes place at the onset of puberty (UNICEF Bangladesh).
The situation of adolescent girls in Bangladesh mirrors that of adult women. It is characterized by inequality and subordination within the family and society. Adolescent boys face other challenges, including poor nutrition, injury, child labour, violence, exploitation, and abuse (UNICEF Bangladesh).Adolescents contribute to society in countless, influential ways.
The adolescent girls situation is particularly complex. Deep-rooted traditions of patriarchy and the subordination of women and girls, make it difficult for adolescent girls to realize their rights in many parts of the world.
Bangladesh’s socio-cultural environment contains pervasive gender discrimination, so girls and women face many obstacles to their development. Girls are often considered
to be financial burdens on their family, and from the time of birth, they receive less investment in their health, care and education. With the advent of puberty, differences in the ways that adolescent girls and boys are treated become much more pronounced. Adolescence is not viewed as a distinct phase of life; instead the onset of physical maturity is seen as an abrupt shift from childhood to adulthood. At puberty, girls’ mobility is often restricted, which limits their access to livelihood, learning and recreational and social activities.
Bangladesh’s rates of child marriage and adolescent motherhood are among the highest in the world.Maternal mortality rates also remain extremely high. Poor maternal health is the result of early marriage, women’s malnutrition, a lack of access to and use of medical services and a lack of knowledge and information. Most women give birth without a skilled attendant.
In the home, women’s mobility is greatly limited and their decision-making power is often restricted. For instance, about 48 per cent of Bangladeshi women say that their husbands alone make decisions about their health, while 35 per cent say that their husbands alone make decisions regarding visits to family and friends (UNICEF, State of the World’s Children) and (Women and girls in Bangladesh).
Age distribution figure
 Growth and development of adolescence period
Growth and development of adolescence period
Adolescence is the period in human development that occurs between the beginning of puberty and adulthood. Growing into an adult is fraught with many moments of pseudo adult behavior with hasty retreats to being a needy child requiring adult guidance and support. With the advent of hormonal development and sexual maturation, comes the task of learning to accept full responsibility for one self.
The onset of puberty generally occurs around age 10-12 in girls and 12-14 in boys. During adolescence body composition also shifts, with girls increasing their percentage of fat and adding curves, while boys tend to increase protein and muscle development. Young men may gain 7-9 kilograms in weight and grow 10-12 cm in height per year, while girls may add 6-8 kilograms in weight and grow 8-10 cm yearly. The main years of growth are between ages 11-16 for girls, and 13-18 years for boys. It must be emphasized here, that the timing and speed of these changes vary with each person and are effected by both genetic influences and environment (nutrition-during-adolescence).
The teenage years are trying times in many ways, especially in terms of nutrition. Rapid hormonal changes and the resulting physiological changes as well as the stresses of ‘growing up’ result in the bodies increased cellular activity and subsequently, the increased need for specific nutrients. This greater demand for nutrients is often met with poor food choices, unhealthy eating habits, and deficient intakes of kilojoules and protein as well as many crucial vitamins and minerals.
The nutritional problems of adolescence are probably related to the rebellious nature of these years. Teenagers eat what they want and when; they are difficult to feed and harder to influence regarding dietary changes. Peer pressure is great. They often have limited food intake – this applies particularly girls who have poor body images and are constantly on diet. The formation of voluptuous and womanly curves increases weight concerns for some girls. Obesity in adolescence usually results from poor food choices and lack of exercise. With increased kilojoule intake during these growth years, there is an increase in the number and size of fat cells. This can lead to lifelong weight problems. Dietary changes, sensible eating and exercise are the best ways to counteract excessive weight gain. Like eating habits, exercise habits are often created early in life, and once set, are harder to change (nutrition-during-adolescence). This is also true for attitudes towards health and life. These factors – eating and exercise patterns, and attitudes are all important in generating long-term health. Boys generally tend to eat enough food, but they may be deficient in nutrients because they often avoid vegetables, whole grains and other whole foods. Fortunately, though, for many teenagers the great demands for nutrients to support growth will increase their appetite for more concentrated protein foods and nutrient-rich foods.
The typical teenage diet is high in refined foods, fried foods, fast foods and junk foods, leading to malnutrition and many common teenage problems. These include acne, obesity, mental and behavioral problems.
Teenagers need to realize the importance of good nutrition, which can help a great deal in promoting healthy looking skin. Dental caries are more common in adolescence, probably due to hormonal changes, a poor diet high in refined carbohydrates (sugars), and mineral deficiencies. A more wholesome diet along with regular brushing and flossing will also promote healthy teeth.
We can help adolescent children best by being understanding and supportive. Our advice should be mild, with suggestions for modifications such as avoiding certain foods and trying others. Parents can be good influences by being good examples, eating well themselves, and not buying refined snack foods for the home. Keeping nourishing snack foods such as fresh and dried fruits, carrots, plain popcorn, nuts and yoghurt on hand, and preparing wholesome meals will help youngsters to make the best food choices.
Nutritional supplementation is of vital importance during the teenage years, as this is when the cumulative effects of below optimum nutrition start to manifest, and worsen into adulthood.
Nutritional needs of adolescent’s girls
“Nutrition is a fundamental pillar of human life, health and development across the entire life span. From the earliest stages of fetal development, at birth, through infancy, childhood, adolescence, and into adulthood and old age, proper food and good nutrition are essential for survival, physical growth, mental development, performance and productivity, health and well-being. It is an essential foundation of human and national development.” (WHO, 2000)
The World Health Organization views nutrition as a fundamental human right that supports and influences every stage of life, at every level of being. It is within this broad context that the relationships between health outcomes, nutrition and school life are viewed. There are several potential impacts of diet on learning.
The importance of managing diet for adults is frequently addressed and has historically been the focus of public health initiatives. Recent research has highlighted the importance of addressing diet in childhood and adolescence, as the precursors to disease have been traced back to very early in life warranting public health attention (Must, 1996; van Kries et al., 1999; Freedman et al., 2001; Pinhas-Hamiel et al., 1996; Wanless, 2004). As such, the diet of children has risen to the top of the political agenda, not only for the impact nutritional intake has for health outcomes later in life, but also for the immediate implications for the physical health, mental health, and overall wellbeing of children (Annik Sorhaindo and Leon Feinstein et al).
The period of adolescence is a time of very rapid growth and high demands for nutrients and energy. The rapid growth period starts at the age of 10 or 11 for girls and at the age of 12 or 13 for boys and continues for about 2.5 years. Adolescents need high intakes of calories, vitamins and minerals, especially iron, calcium, vitamins A, C and D. During this time, boys and girls begin to reach puberty (gaining sex characteristics to mature into men and women) and nutritional needs start to differ, although good nutrition is essential for both sexes to grow into healthy adults. It is important for adolescents to select their foods carefully to ensure that their nutrient and calorie needs are met. When this is the case, their needs for energy (calories) for the additional work they are doing, along with their needs for growth, will have to be met. Some adolescents, however, become less physically active and have to meet their nutrient needs without eating more calories than they need to maintain a healthy body weight.
Adolescence is a time to reinforce good food habits and establish regular meal patterns. Dietary habits and food preferences are developed in childhood and particularly in adolescence. As they become more independent, many adolescents begin to have more meals away from the family, often resulting in poor food choices, skipped meals, increased snacking instead of regular, balanced meals and lower vitamin and mineral intake at a time when good nutrition is especially important. Adolescents also tend to follow food fads and slimming diets which do not meet all of their nutritional needs. It is important at this age to eat a variety of foods, including carbohydrates, plentiful fruits and vegetables, daily protein and dairy foods or other foods containing calcium and to avoid excess fat and sugar. (Nutrition report, part 4)
Adolescent girls
Special attention should be given to adolescent girls, who need to be well-nourished for their own immediate development and for the future nutritional demands of childbearing. Adolescence is a critical time for young women, building the foundation for successful reproduction and a healthy adulthood and later life. Young women must enter adulthood with good nutritional stores to remain strong and healthy throughout their child-bearing years and into old age. Good nutrition is especially important for adolescent girls to meet future needs of pregnancy and breastfeeding.
Adolescence is also the time that the skeletal system builds its strong foundation of calcium stores. If the calcium stores in the bones are not sufficient entering into the reproductive years, bones can become weak with successive pregnancies, leading to broken bones and disability in later years (a condition called osteoporosis). Increasing calcium consumption by eating a diet rich in dairy foods and leafy green vegetables will help meet the increased needs of adolescents for calcium. Because of the demands of growth, as well as blood loss with menstruation, the requirement for iron among adolescent girls is very high. It is important for girls to increase their consumption of iron-rich foods, such as red meats, fish, poultry and legumes, to help prevent anemia resulting from iron deficiency. Adolescent girls who are anemic and may not be eating sufficient quantity of iron-rich foods to meet their needs may be advised, under the guidance of a doctor or other health professional, to take iron supplements.
Early pregnancies can be harmful to the health of girls who, themselves, are still growing. Young girls’ bodies are still developing and usually are not ready to support the extra burden of pregnancy and child birth. Special care must be taken during adolescent pregnancy to insure that the young mother receives sufficient food for her own increased needs, as well as for the needs of the unborn baby.
Nutritional requirement during adolescence
The phenomenal growth that occurs in adolescence, second only to that in the first year of life, creates increased demands for energy and nutrients. Total nutrient needs are higher during adolescence than any other time in the lifecycle. Nutrition and physical growth are integrally related; optimal nutrition is a requisite for achieving full growth potential. Failure to consume an adequate diet at this time can result in delayed sexual maturation and can arrest or slow linear growth(Story M. et al, 1992).
Nutrition is also important during this time to help prevent adult diet-related chronic diseases, such as cardiovascular disease, cancer, and osteoporosis (Stang J. et al, 2005).
Prior to puberty, nutrient needs are similar for boys and girls. It is during puberty that body composition and biologic changes emerge which affect gender-specific nutrient needs. Nutrient needs for both males and females increase sharply during adolescence.1 Nutrient needs parallel the rate of growth, with the greatest nutrient demands occurring during the peak velocity of growth. At the peak of the adolescent growth spurt, the nutritional requirements may be twice as high as those of the remaining period of adolescence (Forbes GR. et al, 1992).
Nutritional requirements vary between individuals and at different stages in the life course. For example, they vary with age, gender and state of health. Individual requirements depend not only on how much of a particular nutrient the respondent needs to successfully digest, but also on their ability to absorb and make use of each type of nutrient. Thus, a range of suggestions are published for required nutritional intake for various populations (British Nutrition Foundation, 2005).
Dietary Reference Intakes
Dietary reference intakes (DRIs) developed by the Food and Nutrition Board of the Institute of Medicine provide quantitative estimates of nutrient intakes to be used for planning and assessing diets for healthy people. The DRIs replace and expand upon the Recommended Dietary Allowances (RDAs). The DRIs contain four categories of recommendations for nutrient reference values (Forbes GR. et al, 1992):
• Recommended Dietary Allowance (RDA): The average daily dietary intake level that is sufficient to meet the nutrient requirement of nearly all (97-98%) healthy individuals in an age and gender-specific group.
• Adequate Intake (AI): A recommended intake value based on observed or experimentally determined approximations or estimates of nutrient intake by a group of healthy people that are assumed to be adequate— used when an RDA cannot be determined.
•Tolerable Upper Intake Level (UL): The highest level of daily nutrient intake that is likely to pose no risk of adverse health effects for almost all individuals in the general population. As intake increases above the UL, the potential risk of adverse effects increases.
Estimated Average Requirement (EAR): A daily nutrient intake value that is estimated to meet the requirement of half of the healthy individuals in an age and gender group. Used to determine dietary adequacy of populations but not for individuals.
Energy and nutrient needs
Energy
Energy needs of adolescents are influenced by activity level, basal metabolic rate, and increased requirements to support pubertal growth and development. Basal metabolic rate is closely associated with the amount of lean body mass. Due to the wide variability in the timing of growth and maturation among adolescents, the calculation of energy needs based on height will provide a better estimate than total daily caloric recommendation (Gong EJ et al, 1994).
The DRI for energy is based upon the assumption of a light to moderate activity level. Adolescents who participate in competitive sports and those who are more physically active than average may require additional energy to meet their daily caloric needs. Adolescents who are not physically active and those who have chronic or handicapping conditions that limit mobility will require less energy to meet their needs.
Protein
Protein needs of adolescents are influenced by the amount of protein required for maintenance of existing lean body mass and accrual of additional lean body mass during the adolescent growth spurt. Protein requirements per unit of height are highest for females in the 11 to 14 year age range and for males in the 15 to 18 year age range, corresponding to the usual timing of peak height velocity. When protein intakes are consistently inadequate, reductions in linear growth, delays in sexual maturation and reduced accumulation of lean body mass may be seen.
National data suggest that on average, teens consume about twice the recommended level of protein and 31% of adolescent boys 14-18 years of age consume more than twice the RDA for protein (Gleason P & Suitor C. et al, 2001).Subgroups of adolescents who may be at risk for marginal or low protein intakes include those from food-insecure households, those who severely restrict calories, and vegans.
Carbohydrates
Carbohydrate is the body’s primary source of dietary energy. Carbohydrate-rich foods, such as fruit, vegetables, whole grains, and legumes are also the main source of dietary fiber. Dietary recommendations suggest that 50% or more of total daily calories should come from carbohydrate, with no more than 10-25% of calories derived from sweeteners, such as sucrose and high fructose corn syrup. Adolescents consume approximately 53% of their calories as carbohydrate (Devaney BL et al, 1995). Foods that contribute the most carbohydrate to the diets of adolescents include (in descending order) yeast bread, soft drinks, milk, ready-to-eat cereal, and foods such as cakes, cookies, quick breads, donuts, sugars, syrups, and jams.
Sweeteners and added sugars provide approximately 20% of total calories to the diets of adolescents. Mean intake of added sugars ranges from 23 teaspoons/day (nearly 1/2 cup) for females ages 9-18 to 36 teaspoons/day (3/4 cup) for males ages 14 to 18. (Gleason P & Suitor C. et al, 2001). Soft drinks are a major source of added sweeteners in the diets of adolescents, accounting for over 12% of all carbohydrate consumed. Soft drink consumption has steadily increased over the years among adolescents.
Fat
The human body requires dietary fat and essential fatty acids for normal growth and development. The Dietary Guidelines for Americans recommend that adolescents consume no more than 30% of calories from fat, with no more than 10% of calories derived from saturated fat. The DRIs do not list specific requirements for total fat intake, but do make recommendations for the intake of linoleic (n-6) and α-linolenic (n-3) polyunsaturated fatty acids. Studies consistently show that adolescents’ intakes of total fat and saturated fat exceed recommendations (Gleason P & Suitor C. et al, 2001). Dietary 24-hour recall data from NHANES III (1988-94) showed the mean percentage of energy for adolescents ages 12-19 was about 34% from total fat and 12% from saturated fat (Troiano RP & Briefel RR et al,2000). There were no differences by gender.
Minerals
Calcium
Calcium needs during adolescence are greater than they are in either childhood or adulthood because of the dramatic increase in skeletal growth. Because about 45% of peak bone mass is attained during adolescence, adequate calcium intake is important for the development of dense bone mass and the reduction of the lifetime risk of fractures and osteoporosis (American Academy of Pediatrics, Pediatrics 1999).
By age 17, adolescents have attained approximately 90% of their adult bone mass. Thus, adolescence represents a “window of opportunity” for optimal bone development and future health. The DRI for calcium for 9 to 18 year olds is 1300 mg/day. Only 19% or about 2 out of 10 adolescent girls meet their calcium recommendations. In NHANES III, the mean calcium intake of adolescent girl’s ages 12-15 was 796 mg/day and 822 mg/day for ages 16-19 (Alaimo K, et al. Adv Data 1994). Milk provides the greatest amount of calcium in the diets of adolescents, followed by cheese, ice cream and frozen yogurt. Calcium-fortified foods are widely available and can be excellent sources of calcium; many of these foods are fortified to the same level as milk (300 mg/serving).
The efficiency of absorption of calcium from supplements is greatest when calcium is taken with food in doses of not more than 500 mg. Many adolescents with lactose intolerance can tolerate small amounts of milk, especially when consumed with meals.
Iron
Iron is vital for transporting oxygen in the bloodstream and for preventing anemia. For both male and female adolescents, the need for iron increases with rapid growth and the expansion of blood volume and muscle mass. The onset of menstruation imposes additional iron needs for girls. Iron needs are highest during the adolescent growth spurt in males and after menarche in females. The RDA for iron is 8 mg/day for 9-13 year olds, 11 mg/day for males ages 14-18 and 15 mg/day for females ages 14-18.
Estimates of iron deficiency among adolescents are 3-4% for males and females ages 11-14, 6-7% for females ages 15-19, and 0.6% for males ages 15-19.27 Rates of iron deficiency tend to be higher in adolescents from low-income families.
National data suggest that most adolescent males (98%) met recommended dietary intake guidelines for iron, but only about half (56%) of females ages 14-18 had adequate intakes. The most common dietary sources of iron in diets of adolescents included ready-to-eat cereal, bread, and beef. The availability of dietary iron for absorption and utilization by the body varies by its form. Heme iron, which is found in meat, fish, and poultry, is highly bioavailable while nonheme iron, found predominantly in grains, is much less so. More than 80% of the iron consumed is in the form of nonheme iron. Bioavailability of nonheme iron can be enhanced by consuming it with heme sources of iron or vitamin C. Because the absorption of iron from plant foods is low, vegetarians need to consume twice as much iron to meet their daily requirement.
Zinc
Zinc is associated with more than 100 specific enzymes and is vital for protein formation and gene expression. Zinc is important in adolescence because of its role in growth and sexual maturation. Males who are zinc deficient experience growth failure and delayed sexual development. It is known that serum zinc levels decline in response to the rapid growth and hormonal changes that occur during adolescence. Serum zinc levels indicative of mild zinc deficiency (<10.71 umol/L) have been found in 18% to 33% of female adolescents (Donovan UM, et al, 1995). The RDA for zinc for males and females ages 9-13 is 8 mg/day. For males and females ages 14-18, the RDA is 11 mg/day and 9 mg/day, respectively.
Zinc is naturally abundant in red meats, shellfish, and whole grains. Indigestible fibers found in many plant-based sources of zinc can inhibit its absorption. Zinc and iron compete for absorption, so elevated intakes of one can reduce the absorption of the other. Adolescents who take iron supplements may be at increased risk of developing mild zinc deficiency if iron intake is over twice as high as that of zinc. Vegetarians, particularly vegans, and teens who do not consume many animal-derived products are at highest risk for low intakes of zinc.
Vitamins
Vitamin A
Besides being important for normal vision, vitamin A plays a vital role in reproduction, growth, and immune function ( Russell RM. Et al, 2001).To ensure adequate body stores of vitamin A, boys and girls ages 9-13 should consume 600 μg/day, females ages 14-18, 700 μg/day and males ages 14-18, 900 μg/day.
The most obvious symptom of inadequate vitamin A consumption is vision impairment, especially night blindness, which occurs after vitamin A stores have been depleted.28 Vision impairment caused by inadequate vitamin A is rarely seen in the US. However, up to 500,000 children in developing countries go blind each year because of vitamin A deficiency.
Vitamin E
Vitamin E is well known for its antioxidant properties, which become increasingly important as body mass expands during adolescence. The RDA for vitamin E for 9-13 year olds is 11 mg/day and 15 mg/day for 14-18 year olds. There are few data available on the vitamin E status of adolescents. National nutrition surveys suggest that dietary intakes of vitamin E are below recommended levels.
Among adolescents the five most commonly consumed sources of vitamin E are margarine, cakes/quick breads/donuts, salad dressings/mayonnaise, nuts/seeds, and tomatoes (Subar AF, et al, 1998). Increasing adolescent intakes of vitamin E through dietary sources is a challenge, given that many of the sources of vitamin E are high fat foods.
Vitamin C
Vitamin C is involved in the synthesis of collagen and other connective tissues. For this reason, vitamin C is an important nutrient during adolescent growth and development. The RDA for vitamin C is 45 mg/day for 9-13 year olds, 75 mg/day for males ages 14-18 and 65 mg/day for females ages 14-18. Almost 90% of vitamin C in the typical diet comes from fruits and vegetables, with citrus fruits, tomatoes and potatoes being major contributors. The five most common sources of vitamin C among adolescents are orange and grapefruit juice, fruit drinks, ready-to-eat cereals, tomatoes, and white potatoes.
Other Food Components
Fiber
Dietary fiber is important for normal bowel function, and may play a role in the prevention of chronic diseases, such as certain cancers, coronary artery disease, and type 2 diabetes mellitus. Adequate fiber intake is also thought to reduce serum cholesterol levels, moderate blood sugar levels, and reduce the risk of obesity. A factor of 10 is added to age to determine the recommended upper limit of fiber intake. Adolescents’ mean fiber intake is well below the age-adjusted target goal. National data show that mean daily fiber intake among girls ages 9-18 is only 12 g, and among males 9-18 years of age it is 15 g. significant sources of fiber in the diet of adolescents include whole grain breads, ready-to-eat cereal.
Cholesterol and sodium
Mean cholesterol and sodium intakes increase with age for both males and females. Males ages 14- 18 have a mean cholesterol intake of 320 mg/day, which exceeds the goal of 300 mg/day. The suggested sodium intake is 2400 mg/day. Average intake for both adolescent males and females exceeds this target.
Diagram of the Food Guide Pyramid
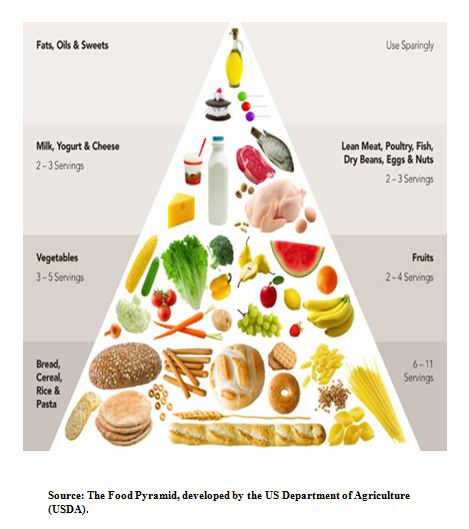
 The Food Pyramid, developed by the US Department of Agriculture (USDA).
The Food Pyramid, developed by the US Department of Agriculture (USDA).
It is a great tool to assist you in making healthy food choices. The food pyramid can assist you in selecting from a variety of different foods so you receive the nutrients your body needs. The suggested portion sizes help control the intake of calories, fat, saturated fat, cholesterol, sugar or sodium in your diet.
Food pyramid for adolescent
 Effects of nutrition
Effects of nutrition
It is difficult to discuss the effects of nutrition on physical, cognitive and behavioral development separately, as nutritional outcomes typically cut across several areas of maturation. Focus on the impact of nutrition on: physical development, with an emphasis on the growing epidemic of obesity; cognition; behavior; and school life.
Nutrition and physical development
This section is the most challenging to tease away from other nutritional outcomes. Physical development is mediated by cognitive development as, generally, nutritional deficiencies first affect the brain then manifest in physical outcomes.
Sight, hearing and speech
Throughout the report, the importance of sufficient intake of highly unsaturated fatty acids (HUFAs) is apparent. HUFAs are important for many areas of physical development, particularly cardiovascular health and immunity. Deficiencies are implicated in a number of neurodevelopment disorders (Richardson and Puri, 2002).
A further trial, testing the efficacy of HUFA supplements in improving ADHD related problems (including dyslexia) among 41 children also demonstrated considerable benefits (Richardson and Puri, 2002).
Motor skills
As mentioned above, dyspraxia, or developmental coordination disorder, and other overlapping neurodevelopment disorders are associated with highly polyunsaturated fatty acid deficiency. Dyspraxia affects approximately 5 per cent of school-aged children and results in impairments of motor function, independent of general ability (Richardson, 2002). Dyslexia and dyspraxia share many common characteristics. Both manifest difficulties with spelling, handwriting and written expression. Research in Durham, UK with 117 children between the ages of 5 and 12 diagnosed with dyspraxia found marked improvements in reading, spelling, and behavior after 3 months of dietary fatty acid supplements, but no effect on motor skills (Richardson and Montgomery, 2005).
Skeletal development
Bone density in youth can determine vulnerability to osteoporosis and fractures in old age. Development in adolescence is the final opportunity to improve bone density before consolidation of the skeleton. Bone density is affected by a number of factors including nutrition. Analysis of cross-sectional data of about 1200 adolescents in Northern Ireland found that high intake of fruits was significantly related to elevated bone density in 12-year old girls even when controlling for potential confounders. As women are more susceptible to osteoporosis, this finding presents a cost-effective public health opportunity for reducing vulnerability to the disease later in life (McGartland et al., 2004).
Body mass index and obesity
Obesity is the most frequently occurring nutritional disorder among children, and is a major risk factor for cardiovascular disease in adulthood (Freedman et al., 2001).Obesity occurs when energy is consumed in excess of what the body can use. To measure obesity the Body Mass Index (BMI), weight (kg) divided by height squared (m2), is determined. Using this classification, a measurement of BMI above the 85 percentile corresponds to overweight and above the 95 percentile is defined as obese (Jotangia et al., 2005). However, internationally acceptable measures that take into account cut-off points widely used in determining overweight and obesity in adults are being developed for children (Cole et al., 2005).
Overweight and obesity in childhood has a number of adverse short-term and long term health implications. Contrary to common belief, many of the effects of childhood obesity are observable in youth. A review conducted by Must and Strauss (1999) listed several immediate consequences including the development of gallstones, sleep apnoea and increased intracranial pressure. They state that young obese women experience a change in hormone development that delays menarche.
Central fatness is a measure of adiposity linked to the determination of cardiovascular disease. Obesity is implicated in the development of insulin resistance limiting the body’s ability to absorb glucose (Hannon et al., 2005). Early reduction of overweight and obesity can improve outcomes later in life (Viner and Cole (2005). Recently found that obesity limited to childhood has little impact on socio-economic, educational, social, and psychological outcomes in adult life.
In addition to the physical health implications for overweight and obesity, there are a number of important social and psychological implications discussed later in this report.
Obesity
Obesity can be a problem for both sexes, and overweight youngsters should be encouraged to increase physical activity and adopt healthier eating habits. Obesity is a nutritional disorder that is becoming more common. Obesity can have devastating consequences for health and happiness. On an emotional level it can lead to a lack of self-esteem and depression. There is no magic cure for obesity, but you can achieve a lower, healthier weight by increasing your level of physical activity and reducing your intake of kilojoules – particularly those that are derived from fat. Parents can be most helpful by packing a nutritious, non-fattening lunch for school, instead of giving money to be spent at the tuck-shop.
Anorexia Nervosa
Though anorexia nervosa mainly effects teenage girls and young women, about one in ten of all anorexics are boys and young men. This complex psychiatric disorder manifests itself as an obsession to limit food intake and is often spurred by a sense of low self-esteem. An anorexic tries to rise above the appetites and problems of everyday life by pursuing a course of food deprivation – to the point of starvation.
Early signs of anorexia, such as an abnormal concern with weight, growing pickiness at mealtimes and obsessive exercising, often occur before the disorder takes hold. Promoting a balanced diet during puberty is particularly important. Anorexics equate extreme slimness with beauty and think that they are overweight when, in fact, they may be dangerously undernourished.
Bulimia Nervosa
Victims of this psychiatric disorder are trapped in a cycle of starving, bingeing and vomiting, and need to gain control of their eating habits. Treatment in a clinic focuses on the establishment of three, regular, nutritious meals a day, avoiding the high-fat and high-sugar fast foods that are often eaten during binges. Bulimics may also need reassuring that a healthy appetite is normal.
Self-induced vomiting, and the excessive use of diuretics and laxatives associated with bulimia disturb the body’s serum electrolyte level (the ions including sodium and potassium which circulate in the blood). This may lead to serious dehydration and produce a potassium deficiency which can cause poor kidney function, weak muscles and irregular heartbeat. Early treatment often entails a diet to restore a normal balance.
The overall goal is to pursuade the sufferer to adopt a healthy eating pattern which includes a wide range of foods. A diet high in fibre will help the movement of food through the digestive system and cut out dependence on laxatives.
Acne
Acne starts when the sebaceous glands overproduce oil, or sebum, secreted through the pores. Sebum carries dead cell debris away with it, but it’s over production blocks the pores with a sticky mass of oil and dead cells. When this happens, the bacteria normally present in skin convert the mass into compounds that irritate and rupture small glands, causing inflammation and unattractive pustules. Some people are genetically predisposed to acne, but the most common causes are emotional stress and increased activity of sex hormones. These hormones stimulate the oil glands – and are especially active during puberty.
Dietary diversity
Dietary diversity is a qualitative measure of food consumption that reflects household access to a variety of foods, and is also a proxy for nutrient adequacy of the diet of individuals. The dietary diversity questionnaire represents a rapid, user-friendly and easily administered low-cost assessment tool.
The dietary diversity scores described in these guidelines consist of a simple count of food groups that a household or an individual has consumed over the preceding 24 hours. The guidelines describe the use of the dietary diversity questionnaire at both the household and individual level, for which calculation of the score is slightly different in each case. The household dietary diversity score (HDDS) is meant to reflect, in a snapshot form, the economic ability of a household to access a variety of foods. Studies have shown that an increase in dietary diversity is associated with socio-economic status and household food security (household energy availability) (Hoddinot and Yohannes, 2002; Hatloy et al., 2000).
DDS were calculated by summing the number of unique food groups consumed by the child in the 24-h period. An all inclusive DDS was calculated without a minimum intake for the food group. A second DDS was calculated applying a 10-g minimum intake for all food groups (DDS 10g) except fats and oils.
Individual dietary diversity scores aim to reflect nutrient adequacy. Studies in different age groups have shown that an increase in individual dietary diversity score is related to increased nutrient adequacy of the diet. Dietary diversity scores have been validated for several age/sex groups as proxy measures for macro and/ or micronutrient adequacy of the diet. Scores have been positively correlated with adequate micronutrient density of complementary foods for infants and young children (FANTA, 2006), and macronutrient and micronutrient adequacy of the diet for non breast-fed children (Hatloy et al., 1998; Kennedy et al., 2007) adolescents (Mirmiran et al., 2004) and adults ( Arimond et al., 2010).
Some of these validation studies refer to only one country while others have attempted to validate dietary diversity scores for several countries. Nevertheless, research is ongoing and there is currently no international consensus on which food groups to include in the scores at the individual level for different age/sex groups.
The Dietary Diversity Scores
The HDDS and WDDS are calculated based upon different numbers of food groups because the scores are used for different purposes. The HDDS is meant to provide an indication of household economic access to food, thus items that require household resources to obtain, such as condiments, sugar and sugary foods, and beverages, are included in the score. Individual scores are meant to reflect the nutritional quality of the diet. The WDDS reflects the probability of micronutrient adequacy of the diet and therefore food groups included in the score are tailored towards this purpose. Previous research has shown that the fats and oils food group does not contribute to the micronutrient density of the diet and this food group is not part of the WDDS.
However, it is important to calculate the proportion of individuals consuming fats and oils as a separate indicator because oil is an important contributor to energy density and improves the absorption of plant source carotenoids and fat-soluble vitamins. Twelve food groups are proposed for the HDDS, while nine food groups are proposed for the WDDS.
As a check on the creation of the DDS variables, all scores should be within the following range:
• HDDS (0-12)
• WDDS (0-9)
The Dietary Diversity Scores Level
- Low dietary diversity scores (< 3 food groups)
- Medium dietary diversity scores (4-5 food groups)
- High dietary diversity scores (> 6 food groups)
Food consumption score
The Food Consumption Score (FCS) is a proxy indicator of household food security based on the weighted frequency (no. of days in a week) of intake of 8 different food groups. Food Consumption Score (FCS) and the classification of food security status based on the FCS.FCS capture both quality (different food groups/dietary diversity) and quantity (food frequency) elements of food security.
The FCS is the sum of the product of frequency of consumption of different food groups by households during seven days before the survey and assigned weight of the food group. The FCS is constructed as follows:
Information on the frequency of household food intake is collected using a country-specific list of food items and food groups. The households are asked about the number of days a given food item was consumed over a recall period of the past seven days. The items are grouped into eight standard food groups. Each group has a maximum value of seven days per week. The consumption frequency of each food group is multiplied by an assigned weight based on the nutrient content of a portion of the food group. Those values are then summed to obtain the FCS. The FCS has a theoretical range from 0 to 112. The WFP has defined thresholds to convert the continuous FCS into categories creating three food consumption groups (FCGs): poor, borderline, and acceptable (WFP 2007).
Whether the FCS is a strong proxy for food intake and, hence, food security or not is still in debate. However, results of a recent validation study suggest that it exhibits moderate positive correlation with household dietary energy (Kcal) intake and high positive correlation with other food-security indicators (Wiesmann et al., 2008). Findings of the study also suggest that the FCS redicts better food security of the poor segment of the population, which is the group of interest in terms of humanitarian and development actions. Furthermore, evidence from the literature shows that there is a significant correlation between the diversity of a diet and nutrition adequacy, anthropometry, and socioeconomic status of children and women (Ruel 2003).
In this section, the FCS was, therefore, used as an indicator of household food security. Information on how many months household was food secure was used for classifying the households into transitory and chronic food insecurity.
Measuring household food consumption
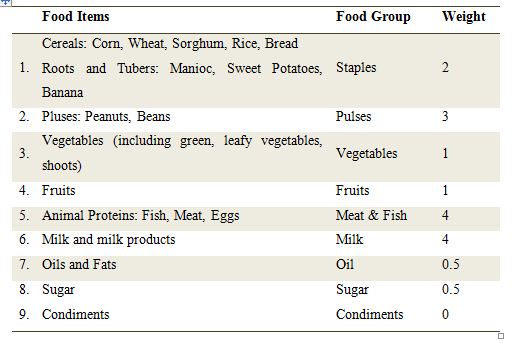
To examine the food consumption pattern, the sample households were asked to mention the number of days they consumed a series of food items in a week before data-collection and the sources of the foods consumed. From a nutrition perspective, different food items were divided into a number of food groups, of which a combination of food groups should be consumed daily to ensure a nutritionally- adequate diet. The key food groups were cereals and tubers, pulses, animal proteins (meat, fish, eggs), vegetables, fruits, milk, sugar, oils or fats, and condiments. For each food group, the frequency or the number of days an item of the food group was consumed was tabulated from 0 (never eaten) to 7 (eaten every day). A weight was assigned to each food group, representing its nutritional importance. The food groups and the weights are presented in following table-
 The WFP have identified two standard thresholds to distinguish different food consumption levels. A score of 21 was set as the minimum food consumption composed by an expected daily consumption of staples (frequency*weight, 7*2=14) and vegetables (7*1=7).
The WFP have identified two standard thresholds to distinguish different food consumption levels. A score of 21 was set as the minimum food consumption composed by an expected daily consumption of staples (frequency*weight, 7*2=14) and vegetables (7*1=7).
- A score below 21 implied that the household was expected not to eat at least staples and vegetables daily and was, therefore, considered to have ’poor food consumption’.
- The second threshold was set at 35, composed by daily consumption of staples and vegetables complemented by a frequent (4 days/week) consumption of oils and pulses (staple*weight+vegetables*weight+oil*weight+pulses*weight=7*2+7*1+4*0.5+4*3=35). With the FCS between 21 and 35, a household was assumed to have ‘borderline food consumption’.
- The households that scored above 35 were estimated to have ‘acceptable food consumption’.
Given the importance of oil and fish in the diet of the Bangladeshi people, these thresholds were modified. The following four food consumption groups were created:
- Poor consumption ( ≤ 28)
- Borderline consumption ( > 28 and ≤ 42)
- Acceptable consumption ( > 42)
An additional threshold was introduced to distinguish the acceptable households between acceptable low (43-52) and acceptable high (> 52).
Knowledge, attitude and practice information
Knowledge, attitude and practice
A KAP survey is a representative study of a specific population to collect information on what is known, believed and done in relation to a particular topic — in this case Adolescent girl’s nutrition. In most KAP surveys, data are collected orally by an interviewer using a structured, standardized questionnaire. These data then can be analyzed quantitatively or qualitatively depending on the objectives and design of the study. A KAP survey can be designed specifically to gather information about Adolescent girl’s nutrition -related topics, but it may also include questions about general health practices and beliefs. (Advocacy, Communication and Social Mobilization for TB control / A guide to developing knowledge, attitude and practice surveys).
Important of KAP survey
KAP survey data are essential to help plan, implement and evaluate ACSM (Advocacy, communication and social mobilization) work. A KAP survey gathers information about what respondents know about adolescent girl’s nutrition, what they think about disease or about the health system, and what they actually do with regard to seeking care or taking other action. KAP surveys can identify knowledge gaps, cultural beliefs, or behavioral patterns that may facilitate understanding and action. They can identify information that is commonly known and attitudes that are commonly held. To some extent, they can identify factors influencing behavior that are not known to most people, reasons for their attitudes, and how and why people practice certain health behaviors. KAP surveys can also assess communication processes and sources that are key to defining effective activities and messages in adolescent girl’s malnutrition prevent. KAP surveys may be used to identify needs, problems and barriers in programme delivery, as well as solutions for improving quality and accessibility of services. A survey could also be designed to explore ways to involve all health providers in adolescent girl’s malnutrition control including outpatient government services, hospitals, and NGOs. The data collected enable programme managers to set adolescent girl’s nutrition programme priorities (e.g. to address the most common problems or to identify specific subgroups whose needs may differ from other groups), to estimate resources required for various activities, to select the most effective communication channels and messages, to establish baseline levels and measure change that results from interventions, and for advocacy (e.g. to show the magnitude of a challenge, which in turn, may inform resource needs). KAP data provide national adolescent girl’s nutrition programme managers and their staff with the fundamental information needed to make strategic decisions.
Situation of adolescent girls of Bangladesh
Nutritional Status
The nutritional status of adolescents in Bangladesh is deplorable. A large number of adolescent girls suffer from malnutrition. The prevalence of malnutrition is found to be markedly higher among female children compared with male children. Short maternal height has been found to account for a sizeable number of low birth weight babies (2.5 kilograms) who are subsequently more susceptible to infections and death in infancy. Those who survive grow up as undernourished adults, giving rise to an intergenerational cycle of undernourishment. Additionally, small pelvis size may cause obstructed labor due to cephalo-pelvic disproportion. The consequences for women range from ill health (from chronic morbidity due to infections of the reproductive system and conditions such as vesico-vaginal fistulae) to death during and after child birth (BNNS, 1998).
Over one-half of adolescent girls are stunted and more than one-third of adolescent girls in rural areas are wasted. Adolescent girls suffer from iron, iodine, and vitamin A deficiencies. Forty-three percent of adolescent girls suffer from iron-deficiency anemia.
Knowledge of nutrition
Knowledge of nutrition among adolescents is poor and they are generally unaware of the need to consume healthy quantities of foods such as fish, meat, eggs, milk, vegetables, and fruits during pregnancy and lactation.
Food Requirements
One study in Bangladesh sought to evaluate adolescents’ understanding about food required for pregnant and lactating mothers: 40 percent mentioned fish, 27.5 percent mentioned meat, 38 percent mentioned eggs, and 34.7 percent mentioned milk. Similar proportions of adolescents mentioned food requirements like meat, fish, eggs, and milk for themselves. The study described above also asked the female guardians (mothers of adolescents) their opinions on whether adolescent girls or boys need to increase their food intake. Of these guardians, 43.1 percent indicated that boys require more food than girls, 19.4 percent indicated that female adolescents need more food, and 37 percent mentioned that the requirement was the same for male and female adolescents.
The reasons for giving more food to girls included that the girls will go to their husbands’ houses and thus will stay with parents for less time (50 percent); the wear and tear on the body due to pregnancy, childbirth, and blood loss during menstruation (2.3 percent); more physical activity/housework (8.2 percent); the need for good health/nutrition (8.2 percent); and having more health problems than men (4.1 percent). The findings of the Bangladesh National Nutrition Survey, 1998 (relating to adolescents ages 10–17) reveal high levels of both stunting and thinness among adolescent girls. Over one-half of girls ages 10– 12 (54 percent) and 13–17 (56 percent) were found to be stunted, with generally higher rates in rural compared with urban areas. A slightly lower proportion of adolescent boys were stunted: 47 and 50 percent for the two age groups, respectively. The Bangladesh National Nutrition Survey, 1998 showed comparative data on energy intake of male and female adolescents. Girls consume fewer calories than boys. They consume 8 percent fewer at ages 10– 12, 18 percent fewer at ages 13–15, and 28 percent fewer at ages 16–19. In terms of meeting energy requirements, boys ages 13–17 consume just enough calories to meet their needs but girls in the same age group have a 4 percent calorie consumption shortage. In the 10–12 year-old age group there is a shortage among both boys and girls. Deficiencies in calorie intake are greater among urban compared with rural girls.
Deficiency Disease
An anemia survey conducted by Helen Keller International (HKI), Bangladesh in rural areas reported that 43 percent of the 200 adolescent girls ages 11–16 who were studied were anemic. (HKI/Bangladesh, IPHN, NIO, and INFS, 1999).
An indication of the prevalence of iodine deficiency disorders (IDD) among male and female adolescents was obtained from a cross-sectional survey in Upazilla of Bangladesh. The survey reported that 3 percent of adolescents had a visible goiter (i.e., an enlarged thyroid). A visible goiter is nearly twice as common among adolescent girls compared with adolescent boys.
A study of approximately 1,000 male and female adolescents (ages 10–17) in a rural area of Bangladesh found that 1.6 percent was suffering from night blindness and 2.1 percent were suffering from physical signs of vitamin A deficiency. A sub-sample of 189 adolescent girls from a large-scale vitamin A survey reported that sub-clinical vitamin A deficiency was found among 12 percent of the adolescent girls ages 12–16.
The community nutrition services under the National Nutrition Project (NNP, Ministry of Health) will be provided to nutritionally vulnerable groups: children younger than two, adolescent girls and pregnant and lactating women. In addition to other core activities, adolescent forums will be formed.
Statement of the problem
In spite of being a signatory to the UN Convention on the Rights of the Child (the development, survival, protection and participation rights of children), Bangladesh has yet to achieve wide acknowledgement and realization of these rights. The barriers to realizing these rights are more prominent in rural areas and in other vulnerable sections of the society. Bangladeshi women, especially adolescent girls, frequently fall victim to gender-based violence in both public and private life. Lack of proper direction and guidance makes it difficult for them to avoid exploitation. Negligence and discrimination in childhood makes them vulnerable and leads them into a life-long downward spiral of deprivation and exclusion from mainstream society. A UNICEF-sponsored study on rural adolescents in Bangladesh states that during the adolescence, loss of mobility, friends, and freedom becomes even more acute for girls ( Tahara et al, 2002).
Adolescence also marks the end of many girls’ formal education, as they are expected to devote their full time to domestic chores in their husbands’ household (Ali and Mohammad, 2010).
Another problem persistent in rural areas of Bangladesh is lack of sufficient and/or well-paying employment opportunities for girls. This lack of opportunity coincides with the cultural tradition of confining young girls/women within the home and teaching them to play passive roles in decision-making, both inside and outside the family context.
Health profile of adolescents
Availability of relevant data and comprehensive analysis of the adolescent sexual and reproductive health (ASRH) situation is necessary for appropriate planning and successful implementation of ASRH strategy. Unfortunately, data related to adolescents and youth people in Bangladesh, as in many other countries, is limited. The aim of this secondary data analysis is to provide knowledge of the health status of different age groups of the young population, showing trends with disaggregated data on sexual and reproductive health indicators from 1993to 2007. The secondary analysis was conducted using all the BDHSs since 1993 to prepare an adolescent and youth health profile of Bangladesh in order to present the existing situation on sexual and reproductive health of young people. The review is limited by the fact that the BDHS currently only collects data form married adolescent women, leaving out data on unmarried women and adolescent men.
Young people aged 10-24 years constitute about 32 % of the Bangladesh population, and urban areas are home to more and more of them. The group of 10-14 year olds has decreased, while the group of 15-24 year olds has increased since 1993/94.
The percentage of 15-19 year old women with completed secondary education has increased by 41 % during 1993-2007, and the percentage of 20-24 year old women with completed secondary education has increased by 30 % during the same period. Employment among young women doubled from 9 % in 1993to 18 % in 2007. Among the poorest 15-19 year olds 75 % were not working in 1993-94, while 21 % said they were in 2007. More women are now being regularly exposed to some form of mass media; however, more than 37 % of 15-19 year old women were still not exposed to any form of media in 2007. (Health Profile of Adolescents and Youth in Bangladesh (gov’t) .1993/94-2007).
Current situation of adolescent girls in Bangladesh
Childhood under nutrition, highly prevalent in South Asia, continues to persist throughout adolescence but little attention has been given to under nutrition of adolescents perhaps for the belief that adolescents are a low-risk group. Stunting in adolescence is 32% in India, 36% in Bangladesh, and 47% in Nepal, and low body mass index (BMI) is 53% in India, 50% in Bangladesh, and 36% in Nepal5. In Bangladesh, 25-27% of adolescent girls are anemic (haemoglobin <12 g/dL) (Ahmed F et al, 1998), and 30% in the age-group of 14-18 years are iron deficient (serum transferring saturation [TS] <15%) (Golden MH et al, 1994) Half (47-54%) of school going children are vitamin A-deficient. The level of zinc deficiency in adolescence is unknown. The average per-capita energy intake by rural adolescent girls is 81% of the recommended dietary allowance (RDA) for age (Public health at a glance adolescent nutrition 2003.)
Protein, iron, and calcium are important for growth spurt and skeletal development in adolescence. More than 60% of schoolgirls aged 10-16 years in Dhaka city consume protein, iron, and calcium less than 75% of the RDA for age. The high prevalence of chronic energy and micronutrient deficiencies of today’s adolescent girls is directly linked to the quality of the next generation. Without addressing these deficiencies, the vicious cycle of inter-generational under nutrition, chronic diseases, and poverty perpetuates ( Jamil KM et al, 2008)
Objective
General Objective
Assess the differential levels in nutritional status, dietary intake and to explore relevant knowledge, attitude and practice of adolescent girls in urban Bangladesh.
Specific Objectives
- To assess their anthropometric data ( height, weight, MUAC)
- To estimate their nutritional status
- To record their 24 hour food intake
- To observe their knowledge about food and nutrition
- To observe their health status knowledge
- To understand their life style practices
Hypothesis
Most of the adolescent girl’s nutritional status (BMI) of urban Bangladesh are not in normal level (>18.5-23) and Knowledge of nutrition among adolescent girl’s is poor.
Rationale
Good nutrition is important to maintain and improve health status the body’s protection against infection and therefore helps girls to stay healthy. Under nutrition among adolescent girls is a serious public health and complex problem internationally, especially in developing countries. In Bangladesh there is few study conduct in this topic of adolescent girls. Adolescent girls under nutrition are one of major public health issue in Bangladesh. Malnourished adolescent girls are at risk for growth development, impact on disease symptom, indicator to chronic dietary inadequacy and micronutrient deficiencies and risk factor for other health problems.
Furthermore the initiatives to provide nutritional care and support for adolescent girls such as those undertaken by NGO and adolescents health service programs are limited in scope and coverage. For these reason nutrition education is important to determine the nutritional status of the adolescent girls. Nutrition education plays a crucial role in the adolescent nutrition service program by helping participants achieve positive changes in nutritional status improve their diet. Nutrition education teacher positive changes in eating habit dietary pattern and knowledge attitude and practice about nutrition and related discuss which keeps then healthy.
This study will help to identify the percentage of urban adolescents girls are malnourished. It will also help to proper health profile of adolescents girls in Bangladesh by nutrition education during the intervention. It will enable programs and nutrition services to provide consistent and sound recommendation and contribute to greater awareness of the importance of nutritional responses of adolescent girls.
The nutrition service programme is designed to address these problems through a program of nutritional supplementation, nutrient adequate, nutrition education adolescent needed health care, social and mantel service.
This study will help to development and adoption of nutrition of dietary requirement and aware the knowledge of nutrition. The study will focus the national, community guidelines and planning are the integration of food and nutrition interventions into adolescent girls nutrition service.
This service will recommend for these NGOs and health organizations, which are working with adolescent girls. Government will also come forward to provide support to adolescent girls by maintaining their good nutritional status and prisoner growth development through regular monitoring. It will lead further studies on this topic.
Study area
The study was conducted in selected five institutes in Dhaka city. The institutes are Agrani school & college; Rahmat ullah model girl’s high school; Azimpur girl’s school & college; Jamila khatun lalbag girl’s high school and College of Home Economics. A total number of participants were randomly selected different classes in those schools.
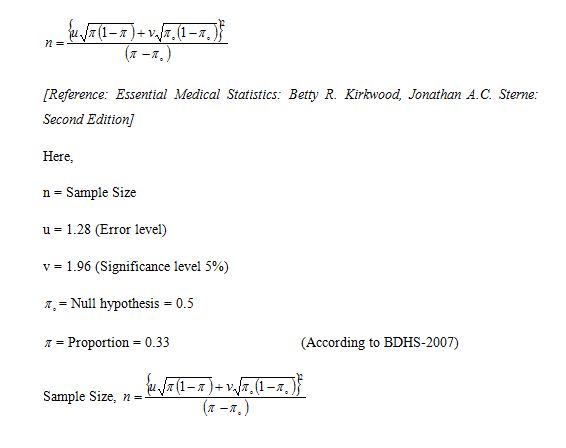
Sample size calculation
Sample size is needed to provide data to determine the nutritional status of the urban adolescent girls.
Efficient sample size calculations are based on an estimate of the sample size required to limit sampling variability to the desired level. Therefore, sample designs other than simple random sampling have an impact, called design effects, on sampling variability. As a result of this impact design effects are important considerations when determining sample size.
More over some urban adolescent girls may not agree to give interview, some are may be too sick to talk and some data may not be completed. So i add dropout 10% with the calculate sample size.
Formula
 Tools use for data collection
Tools use for data collection
Anthropometrics measurement (weight, height and MUAC)
- Weight of the adolescent girls was measured using weighing scale, with a sensitivity of 100g. The weight was measured at least three times. If the scale measured the weight accurately within a precision of 100 g, the scale was selected as the standard to measure the weight.
- Height of the adolescent girls was measured using locally made height scale within a precision of 0.1 cm (1 mm).
- Mid upper arm circumference (MUAC) of the adolescent girls was determined using the TALC (Teaching Aid at Low Cost, St Albans, UK) MUAC tape, with a precision of 1 mm. MUAC was measured at the midpoint between the shoulder and the elbow on the bare left arm using the insertion TALC tape to the nearest cm.
Data on Dietary intake
It is important to assess dietary pattern of any population in order to have a broader idea of nutrient intake and nutritional status of any population. Dietary patterns are the
outcome of meal patterns of the individuals, that are determined from short term individual food or composite foods intake patterns.
- To know the adolescent girls nutritional status was recorded their dietary intake by 24 hr recall method and seven days food frequency questionnaire (FFQ). Adolescent girls asked that to recall all the foods and liquids consumed with amount and frequency in the last 24 hours for measurement of nutrient. Food diary and food frequency questionnaire were pretested before actual collection of food intake data. Therefore the adolescent girls were also evaluated for their food choices with the help of a food frequency questionnaire (FFQ). The most commonly used foods were listed in this FFQ and adolescent girls were asked to tick the eating frequency of each enlisted food.
- Dietary diversity scores data was also collected of the adolescent girls. Dietary diversity was defined as the number of different foods or food groups eaten over a reference time period disregarding the frequency of consumption. Food frequency, in this context, is the frequency (in terms of days of consumption over a reference period) that a specific food item or food group is eaten in the household.
- The Food consumption score is the sum of the product of frequency of consumption of different food groups by households during seven days before the survey and assigned weight of the food group. The FCS is constructed as follows: Information on the frequency of household food intake is collected using a country-specific list of food items and food groups. The adolescent girls are asked about the number of days a given food item was consumed over a recall period of the past seven days.
Data on socio-economic status, personal hygiene
Data on socio demographic information, intake food supplements, personal and hygiene were also collected by structural questionnaire.
Data on their knowledge, attitude and practice about nutrition and health
Data on nutrition and health related information, knowledge of nutritious food, affected various disease conditions (knowledge, attitude and practice) data were collected orally by an interviewer using a structured, standardized questionnaire.
Data Coding Editing and Entry
While the data was collected, I start data editing and coding. After coding data, it was entered using suitable data entry software ( SPSS / PC+).
Data Analysis
Data collected were analyzed with the help of SPSS, version-17 software. Table and graph sand statistical analysis was done by adequate tables and graphs.
Quality control method
Data quality was controlled through tools verification (compare to standard tools) questionnaire, check editing, data entry, entry and minimizing response errors through prove question. Here, use the data collected from dependable sources. Supervisor was also check the filed work for quality.
Development of questionnaire
Before preparation of questionnaire, secondary had been reviewed and drafted the initiation questionnaire. After field test it was finalized.
Field test
Three days field test were conducted after designing the questionnaire. During the field test each individual conduct to interviewers.
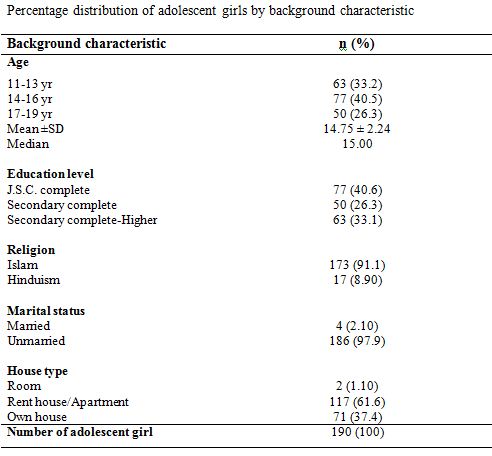
Background information
 SD=Standard deviation
SD=Standard deviation
This table is showing background characteristics of adolescent girls. The subjects are divided into 3 age groups as 11-13 yrs, 14-16 yrs and 17-19 yrs.
Between the age groups of 11-13 yrs the total subjects were 33.2%, the age groups of 14-16 yrs the total subjects were 40.5% and the age groups of 17-19 yrs the total subjects were 26.3%.
The education level of adolescent girls are J.S.C. complete were 40.6%, Secondary complete were 26.3% and Higher Secondary complete were 33.1%.
Among the 190 respondents, 91.1% of respondent’s religions were Islam and 8.90% of respondent’s religions were Hindu.
In the total study participants only 4% were married and also all participants were unmarried.
Among the total study participants only 1.1% were lives in room, 61.6% were lives in rent house/apartment and 37.4% were lives in their own house.
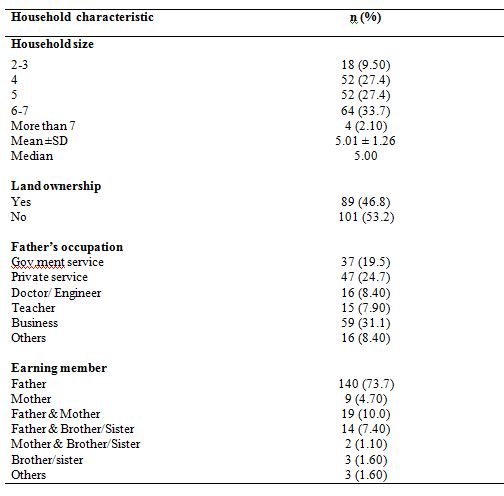
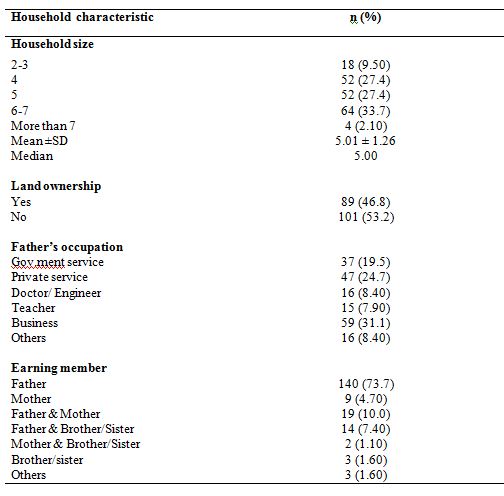
Household information
 SD = Standard deviation
SD = Standard deviation
The table is showing the household characteristics of the study participant.
Numbers of the family member are divided into 4 categories that mean household size. The small household sizes were 9.5% where member was 2-3 people. The medium household sizes same percentage were 27.4% and 27.4% where member was 4 and 5 people. The large household sizes were 33.7% where member was 6-7 people. The Mean (±SD) household sizes were 5.01±1.2 and Median 5.00.
Among the total 190 respondents, 46% have their own land and 53.2% have their no land.
The respondents fathers highest occupation was business and percentage were 31.1% and lowest occupation teacher and percentage were 7.9%.
Most of the adolescent girls earning member of the family was father 73.7% and father & mother both are only 10.0%.
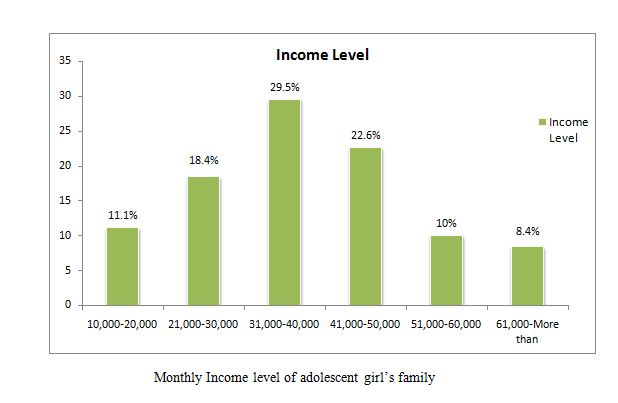 The chart is showing the monthly income of the adolescent girl’s family.
The chart is showing the monthly income of the adolescent girl’s family.
The highest income level was 31,000-40,000 taka & percentage was 29.5%. 11.1% adolescent girl’s family income was 10,000-20,000 taka only. Few (8.4%) adolescent girl’s family income was 61,000- more than taka.
The adolescent girl’s family incomes Mean (± SD) was 40,589± 16,751 and Median was 40,000 taka.
 This figure shows that the percentage of source of the use of water.
This figure shows that the percentage of source of the use of water.
Among the total respondents 100% were used supply water. There were no one use tube-well or other sources water.
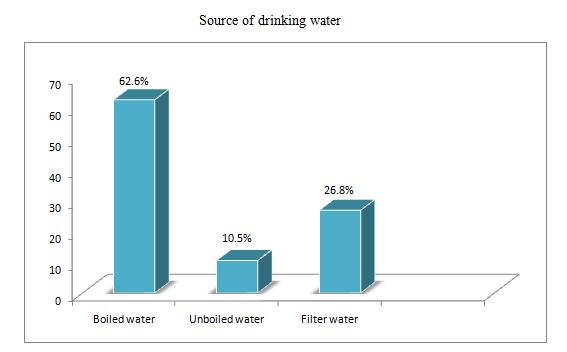 This chart shows that the percentage of source of drinking water.
This chart shows that the percentage of source of drinking water.
There 62.9% were drink boiled water, 10.5% were drink un-boiled water and 26.8% were drink filter water from supply.
 Discussion
Discussion
Adolescence is crucial period for major changes in human body, especially in girls. To supply growth and maintain basic daily needs, adolescent need increased nutrients to provide for the accelerated growth takes place during these years. Under nutrition among adolescent girls is a serious public health problem internationally, especially in developing countries.
Present study represented that nutritional status and dietary intake, and nutrition related knowledge, attitude and practice of urban adolescent girl’s special emphasis was also given to their nutritional status and nutritional need according to the RDA and association nutrition related practice with health status and illness.
In this study focuses intake 7 days food frequency, Dietary diversity score and food consumption score. This study also informed that effect of socio-Economics status with their nutritional status and hygiene practice.
This study was a cross sectional descriptive study and it’s sample size was 190 and the subjects were divided into 3 age groups as 11-13 years were 33.2%, 14-16 years were 40.5%, 17-19 years were 26.3%. In this study among the 190 respondents 91.1% were Muslim and 8.90% were Hindu. Data was collected different schools so all of respondents were student. Most of respondents were complete J.S.C education. Only 4 adolescent girls were married and other all participants were unmarried.
The mean size of house holds with was compared with the different number of the house holds. One-third of the adolescent girl’s house holds size was 6-7 members. It was bigger than the mean size of the house holds with the adolescent girls.
All most 75% house holds main earning member was father and only 10% house holds main earning member was father and mother both of the adolescent girl’s.
One-third participant of father’s occupation was business and it was the highest percentage. On other hand lowest occupation percentage was 8% and it was teacher. Data collective indicate that majority of the participants belonged of the families of moderate to high socio-economic status.
Present study result is showing the mean income of the house holds was Tk 40,589 per month. One third household’s income was equal with the mean income. 30% participant’s income was bellow than the mean of the households and 40% participant’s income was heights than the mean of the households. The land ownership result is consistence with the average monthly income of the adolescent girl’s house holds.
All of the adolescent girl’s house holds used supply water for use. It was good finding two-third of the house holds used boiled water for drinking. Only 10% use un-boiled and 27% used filter water for drinking.
The toilet facility result is consistent with the monthly income of the adolescent girl’s house holds. 57% of the adolescent girl’s house holds use sanitary toilet and 43% of the adolescent girls house holds was flash toilet.
The result of the study revealed that, in urban Bangladesh, the prevalence of under weight was 33% among the adolescent girls (BDHS-2007). This prevalence of under weight in the girls suggested that they were suffering from chronic under nutrition.
The nutritional status of adolescent girls was assessed for thinness and under weight (BMI) and the result were classified by the age. Based on the study result all of the ages of adolescent girls the mean BMI was. Height (cm) was, weight (kg) was and MUAC (cm) was. On average 5% about of the adolescent girls were found sever thinness and 8.2% of the adolescent girls were found moderate thinness. Also using a cut off point of BMI, about 31% of the adolescent girls were found under weight. 54% girls was normal weight, 7.4% was over weight and only 0.5% was obese. These results provide substantial evidence of an overall worse nutritional status in the urban adolescent girls in Bangladesh.
The study observed the mean BMI was compared with NCHS reference value by the age. In the result showed the mean BMI between observed and reference value more difference was 3.33 among the 11 years. Also low difference was 1.91 it was among 13 years adolescent girls. Other the mean BMI difference between observed and reference value was closest 3 it means the poor nutritional status of the adolescent girls.
In the same way the observed mean MUAC was compared with NCHS reference value 19 years adolescent girls mean MUAC difference was highest 6.2 cm among the observed MUAC and reference value MUAC 13 years adolescent girls mean difference was lowest 3.36 cm. The difference rates were little higher in the mean difference of MUAC among the observed and reference value.
This present study results on house hold food security, food consumption score and consumption of food items in the last 7 days.
All the participant house hold ate cereals and oils everyday in the last 7 days. The 7 days food frequency data showed no difference in the intake of rice/wheat among economic groups. The consumption of mean days of protein rich foods such as meat/eggs and milk and products in most of the participants were good, although intake of fish was low in 7 days. Nearly 5 days was the mean intake of pulse by weekly in all adolescent girls. It was observed that considerable proportions of the participants did not take leafy vegetable (27.7%). Present study showed that the participant’s entire vegetable consumption rate was 44.2% and intake mean days of 3 days by weekly. Comparatively the fruit intakes in 7 days were not bad and the percentage was 38.4% and intake mean days of 2 days in 7 days.
All of the participant’s beverage intake percentage was 38.4% and it also observed that 1 day’s beverage intake percentage was 33.7% and 2 days beverage intake percentage was 29.5%. Among study participants mean days of fast food intake was 2 days by weekly and 39.5% participant intake fast food 2 day in 7 days.
This study also observed that all of the participants 23.2% intake food supplement in 7 days and only 11.6% intake nutrient supplement in 7 days.
Nearly 85% adolescent girl’s house holds food consumptions score was acceptable high and that score was > 52. Comparatively low percentage of the participants (8.9%) food consumptions score was poor or borderline and score <=42 other participants were stay in acceptable low level and that score was 43-52.
The study also finding the dietary diversity score of adolescent girls. About three-froths participants consume 4-5 food groups in last 24 hours. All most 75% adolescent girls stay in medium dietary diversity score 7.9% adolescent girls dietary diversity score was low dietary diversity score (<3 food groups) and 17.3% adolescent girls dietary diversity score was high dietary diversity score (>6 food groups).
Adolescent is an important stage of growth and development that requires increased nutrition and anthropometry varies significantly world wide.
The mean energy intake was 1414.27 (kcal/day) with the all age groups of adolescent girls. The energy intake was not sufficient. Intake of carbohydrate by the participants was 242 g/day. This was similar to that of the mean carbohydrate intake (231 g/day) in urban adolescent college grills of Bangladesh. Protein intake the participants was 52 g/day and it was much lower than the RDA. Intake of fat by the participant was 30 g/day and cooking oil is thought to be the major contributor of fat intake.
The study participants were asked to name food items that are rich sources of energy, protein, vitamin, minerals, fat, iron and iodine. In order to assess their knowledge on the nutritive value of different food values.
The results are summarized in general, half of the participants were able to correctly related the foods were able to relate the foods with their nutritive value. Rice, Nearly 80% of the participants said that rice, meat, eggs, milk was an energy dense food.
Most of the participant knew that vegetable fruits were good sources of vitamin and minerals. They could not separately distinguish the vitamin rich foods from the energy dance and protein rich food. They thought that rice, egg, meat and milk were also vitamin rich foods. Most of girls knew that oils in the main source of fats. Fewer participants said the other source of fat food. However one – third of participant could properly identify the vegetable sources of iron rich foods but they had knowledge animal sources of iron. A few of them were confused with the sources of iron and iodine. They knew that salt is the main source of iodine. But all participants’ knowledge on the food values of different food item was good with out iron and iodine rich foods.
Only 11% participants were take iron tablet and 20% take anti-harmonics tablet.
Goiter over 80% of girls who participants in the study heard about goiter and most of them mentioned specially iodine deficiency as the cause of goiter. Half of the participant was known about the role of iodine in causing preventing goiter and 30% were don’t know what the preventing way of goiter is.
The adolescent girls were asked questions on causes of and preventive measures against diarrhea. They mentioned several causes of diarrhoea. The cause most frequently mentioned was eating spoiled or contaminated food, followed by drinking dirty spoiled or contaminated water and dirty environment. Some mentioned not washing hand before eating meals. Knowledge was more prevalent among adolescent girls. They participant mentioned stated several preventive measure against diarrhoea. The measure most frequently stated was taking safe food. Followed by safe drinking water and maintain personal hygiene. Most adolescent girls mentioned use of ORS for the management of diarrhoea.
In this study 90% adolescent girls were aware that vitamin A deficiency is the major cause of night blindness and preventive measure against night blindness was rich. Few participants mentioned other cause of night blindness.
Compared the knowledge a night blindness knowledge of the adolescent girls on anemia was much poor. Nearly 30% of the girls were aware the major causes of anemia and about the role of iron-rich foods in preventing anemia. Other 63% were having no knowledge about the preventive measure against anemia.
One – third of the adolescent girls are suffering from various diseases symptom. The burden was the most common illness being fever cough and common cold. The second most common causes of illness of adolescent girls were the diarrheal diseases in clouding dysentery other cause of illness was ear and eye infection skin and other diseases.
Optimal knowledge and practice regarding personal hygiene are very important to prevent communicable disease such as dysentery diarrheal diseases fever cold skin diseases and others. Most of the adolescent girls 76 % brushed their teeth 2 times daily cat their rails half of the girls 1 weakly 30% cat their rails half of the girls 2 weakly only 17% cut their mail monthly. All of the adolescent girls take bath and washed their hands before and after eating meal. And all most 98% adolescent girls were shoes when they going to toilet while.
Limitation of the study
While conducing this study I had to overcome some obstacles.
- The study had to be limited to a small community due to shortage of time and resources.
- Due to limitation of time sufficient questions could not incorporate in the questionnaire it was not possible to obtain accurate age regarding of the participants.
- Some adolescent girls did not give accurate information about income, knowledge of food values.
- Retailed history of dietary intake was collected through interviews. But the rescores could not observe the quality and quantity of the food consumed and their intake 7 days food frequency.
One limitation of the study that impact on health and growth development by nutrient of adolescent girl’s concept was unclear.
Conclusion
Adolescence is also a sensitive period, particularly for girls. Poor access to proper healthcare, nutrition, and education, as well as vulnerability to sexual abuse and other forms of violence, can have long-term effects on their health and the health of their children and communities.
Results indicate an overall poor nutritional status of the urban adolescent girls in Bangladesh and need for appropriate nutrition interventions to overcome the problem. Findings of the present study indicate that over nutrition or obesity is not the major problem of adolescent girls of capital, rather some are suffering from under nutrition as well. The key challenges for promoting programmes to prevent under nutrition at the national level in Bangladesh include: placing nutrition high up on the list of priorities, implementing cost effective and sustainable interventions at scale following appropriate strategies, improving access to the services for those in real need, and evidence-based decision-making and building up operational capacity. In addition to health and nutrition interventions, economic and social policies addressing poverty, trade, and agriculture that have been associated with rapid improvements in nutritional status should be implemented. Nevertheless, for any nutrition and health intervention to be cost-effective, strong governance is essential. Failing to respond to the population’s need and provide the right services to the right people and weak accountability at all levels of designing through implementation and evaluation would result in unsuccessful efforts. The effects of the development of preferences for and intake of, foods of poor nutritional value early in life can have long-term health implications. Ultimately, the aim must be to prevent such deficiencies from arising, but the relationships between nutrition, health, education and social and cultural factors are complex and multidirectional and do not fully understand the nature of the interactions between these factors. Nonetheless there is evidence that appropriately designed interventions can help to address early deficiencies and engage both children and adolescent in healthy eating. A concerted effort between schools, families, government departments and other agencies is necessary to improve adolescent girl’s nutritional intake.
Recommendation
Adolescence is also a sensitive period, particularly for girls. Poor access to proper healthcare, nutrition, and education, as well as vulnerability to sexual abuse and other forms of violence, can have long-term effects on their health and the health of their children and communities. Adolescence is generally a time of good health but tremendous physical, emotional, and psycho-social growth, which can lead to mental health concerns that are less common in other age groups.
Adolescence is generally a period of extreme social awareness and growing capacity for critical thinking, planning, and decision-making. While adolescents’ social preoccupations can occasionally lead to disruptive behavior, it can also be channeled for positive and healthy purposes. It is suggested that a comprehensive strategy should be implemented in disadvantaged groups of our country in order to prevent adolescent girl undernourishment.
To maintain the proper growth and development and nutritional status of adolescent girl it is necessary to eliminate all those problems associated with inadequate food intake, change dietary pattern, primary health service, personal hygiene condition, proper care, improper nutrition knowledge, inadequate nutrition knowledge etc. In our study some of those qualitative aspects were absent. To remove these constraints some suggestions are offered below-
- Adolescent girls should take calorie rich food and fulfill their RDA.
- To proper growth development and stay well being they should take high biological value protein dance food.
- Nutrition education programs addressing the nutritional status of adolescent girls should be aware of the epidemic problem of poor diet, malnutrition, lack of nutrition knowledge and hygiene practice.
- To maintain household food security and solve economical problem can be very effect to improve their nutritional status.
- Many national, district and community based social and health based organization should recommend improve guidelines for adolescent girls.
- Additional support should be provided to catalyze increased knowledge and attitudinal and behavioral change among service providers with regard to adolescent girls.
- Increased networking between all relevant government organizations and NGOs working with adolescent girls should be encouraged to ensure the proper implementation of projects.
- The government and NGOs should come forward by regular training and monitoring health programs and policies for the adolescent girls.