INTRODUCTION:
There are numerous theories regarding the causes of aging. The rate of aging and normal life span is very variable. Regardless of chronologic age, some physiological changes are inevitable. Age 60 is the period when the body destroyed day by day. There many body changes that results due to the influences of hormones. There happens chewing, digesting, swelling problems. Fewer taste buds and decreased numbers of nerve endings, decreased levels of gastric HCL and pepsin (20%), decreased liver size and blood flow, bacterial overgrowth in proximal intestine, changes in body composition ( reduced muscle mass, increased fat), decreased bio-availability of proteins, vitamins and minerals, mal absorption syndrome, reduce drug tolerance, PCM- these various problems become part of elderly people. The morbidity rate becomes high day by day at this age.
The elderly or older people are the senior citizens of a country. They are very respectable in a family, community and in the state. The elderly population is increasing over the world. According to NIPORT, the statistics shows that 1.13 million people are above 60 years old, which is 7.1% of the total population. It is a matter of fact that in developing socio-economic condition elderly people not get much importance in regards to nutritional status and diet habit which is mandatory for healthy life.
A geriatric person suffers from health and nutritional problems. Geriatric nutrition applies nutrition principles to delay effects of aging and disease to aid in the management of the physical, psychological and psychosocial changes commonly associated with growing old. These problems are caused by overloaded physical activities during the young age, lack of knowledge about nutrition, less food intake, changes in body composition, absence of old age friendly sources of care. People in older age are dependent as a result the study will need to be more careful about their dietary habit. Because elderly people often face chewing, digest problem.
Differential food practices attribute to higher malnutrition among male and female elderly people. Discrimination against female in intra family allocation of food leads to effective malnutrition. In a country likes Bangladesh with verifying social customs and common beliefs against elderly people. In Asian countries female elderly people are much sufferer of malnutrition than male but in a short way to say, both are much sufferer and malnourished highly.
The elderly people suffer malnutrition for various reasons. Some of them are as follows:
- Lack of access education about nutrition.
- Social and cultural environment of Bangladesh.
- Poverty
- Wrong food habit.
- Sickness.
The elderly people face some complications, which are as follows:
- Osteoporosis, osteomalacia
- Hyper homosystenemia
- Heart disease
- Nephrosis
- Diabetes
- Blood pressure
- Amnesia
- Hearing problem.
- Insomnia
The age structure of Bangladesh’s population is changing markedly. Rapid fertility declines in the 1980s have decreased the proportion of young persons (1), and reductions in child mortality have increased life expectancy from 44 years in 1975 to 60 years in 2001 (2). The population aged over 60 years currently represents about 7% of the 140 million population of Bangladesh (1) and is projected to represent 16% of the total population by 2050 (3). As the older population grows, the prevalence of chronic disease is also likely to grow. Understanding the burden of chronic disease in Bangladesh will guide the design of strategies to prevent chronic illness and provide health care to increasingly larger numbers of older people with chronic conditions.
The proportion of participants from each age group included in the survey was similar to the proportion of that age group in the population under surveillance. The majority of respondents lived with extended families. Although life expectancy for men and women in Bangladesh is similar, many more women than men had experienced the loss of a spouse. Smoking was commonly reported by male respondents (Table 1).
Overall, 73% of those surveyed in Mirsarai and 44% in Abhoynagar reported being diagnosed with at least one chronic condition; prevalence varied by sex. (Table 2) Participants most frequently reported being diagnosed with arthritis (54% in Mirsarai, 17% in Abhoynagar) and hypertension (32% in Mirsarai, 20% in Abhoynagar) (Table 2). Women in Mirsarai reported the highest rates of chronic disease (82%).
Evidence from Mirsarai and Abhoynagar suggests that chronic illness is common in persons aged over 60 in Bangladesh. This population-based survey found that 73% of persons aged over 60 were living with at least one chronic disease complaint in Mirsarai and 44% were doing so in Abhoynagar. It is unclear why differences in disease prevalence existed between the two sites surveyed and between males and females; however, other studies have also observed higher proportions of females with chronic illness than men (5, 6, 7). Estimated prevalences reported here and in other studies from Bangladesh based on reported illness (7) are likely to be underestimates given that they are based on participant reports and that this population traditionally has poor access to regular medical care necessary to diagnose chronic illnesses. Studies conducted with similar populations in neighbouring India, which included a physician diagnosis, report that nearly all persons aged over 60 surveyed were living with some morbidity (5). Further studies, including physician exams, are required to accurately document the prevalence of chronic disease in Bangladesh.
Hospitalizations of persons over the age of 60 accounted for only 5% of all hospitalizations in Mirsarai and 7% in Abhoynagar. Despite the fact that most deaths at these facilities in people over 60 are attributed to chronic illness, hospitalizations for this age group for chronic illness were rare. Another study from Bangladesh found similarly low proportions of hospital admissions from this age group (8). This could be explained in a number of ways. It is possible that these people are receiving treatment elsewhere since upazila health complexes usually do not have the resources to treat chronic conditions. Another possibility is that these people simply are not seeking care for their illnesses, either because they do not have the resources to do so or because they are unaware of their condition and the need to seek treatment. Anecdotal evidence suggests that community members are reticent to seek care for older members of the family. While conducting the survey for this study, interviewers were often requested by younger adults in the household to collect information on the health of younger family members instead. They said, “What is the use of collecting such data for older people, as no intervention is likely to bring them back to a normal life. It is better to keep him/her with the family and leave them alone to perform rituals as long as they survive”.
As Bangladesh’s population ages, increasing numbers of people will be living with chronic conditions. The Government of Bangladesh is committed to sustainable improvements in health, nutrition and family welfare especially for vulnerable groups such as the elderly. These commitments are outlined in the Health, Nutrition and Population Sector Programme (2003-2010) (9) and the national Strategy for Accelerated Poverty Reduction (10). Given evidence of the current burden of chronic disease and the predictions for growing numbers of people with chronic illness, the government should work to increase resources for diagnosis and treatment of these conditions and initiate strategies, such as lifestyle change, for preventing them. One step could be to discourage smoking, a common habit among men found in this study and others in Bangladesh. The future holds many challenges for Bangladesh’s health care system, which will have to cope with high rates of infectious disease and increasing rates of chronic disease. Further studies to generate more accurate estimates of the chronic disease burden and track trends will assist the government in facing this challenge.
In the United States, the recent geriatric certification examination jointly administrated by the American board of family practice and the American board of international medicine has caused controversy. The geriatric population represents a continuum of the family life cycle that already belongs within the reclaim to the family physician’s knowledge. The concern of discipline of geriatrics social supports, environmental assessment, occupational status, cognitive function, activities of daily living and physiological changes of organ- system are within the grasp of the practicing family physician. It is clear that majority of physicians who are in internal medicine or family practices are not knowledgeable about some aspects of geriatric medicine, because only 56% 0f 4282 examinees who sat the last examination were successful. Although a large minority failed, more than 90% of those who had some formal training are geriatric passed. These data indicate a need for family physicians to keep up data with the geriatric literature in light of expected increase of sub-population in our practices. The articles reviewed in this selection from current literature were chosen for their relevance based on the prevalence of the issues raised and applicability to any geriatric patient. It is seen that the knowledge and practice of geriatric nutrition is not in accepted level in U.S.A. even (13).
The study can assume the level of awareness in this topic is varying poor in a least development country like Bangladesh. So this research will be benefited for elderly people.
Hypothesis
Objectives
Rational of the study
Hypothesis
The elderly people take significantly less nutrient 30% approximately comparing to RDA.
Objectives
General objectives:
To determine nutritional status and food intake pattern of elderly people living in old home & family.
Specific objectives:
- To find out the food intake pattern of elderly people.
- To identify the nutritional status of geriatric people through height, weight & BMI
- To assess the socio-demographic status of old age people who are living in old home and family.
- To know about the illness of elderly people.
Rationale to the study:
According to the BDHS, 2007 census 7.1% of the population is aged over 60 years (according to NIPOD).
The absolute number being more than thirteen million. Approximately 80,000 people move into this age every year.
Almost 60% of elderly people are malnourished (according to report by Asia Bangladesh). There are no few researches done about geriatric people. This is why this study has been considering with nutritional status. Due to lack nutritional status they are suffering from malnutrition. So it is very need to be upgraded their nutritional status.
The study can make some policy level suggestion so that geriatric people can be benefit in general:
- To improve geriatric health program of Govt.
- To draw attention at geriatric level / old age level.
- First aid treatment and regular health checkup.
Conceptual Frame works
Conceptual Frame works:

METHODOLOGY
Subjects randomly selected elderly people individuals which participated in interviews. Age, sex, socio-demographic status, house hold expenditure on food and self reported health problems were investigated as potential predicators of nutritional status.
The study noted on 24 hours food recall, 7 days food intake pattern, food frequency, height, weight and BMI to understand the nutritional status of individual.
Age group: The study included ≥60 year’s old people.
Sex: Both male and female.
Study design
The study was based on cross-sectional descriptive study of male and female with family and old home.
Inclusion Criteria
- Elderly people, who are available in old home and selected residential area.
- Those who are interested to give interview.
- Minimum one month staying in old home.
- Those who are ≥60 year’s old people.
Exclusion Criteria
- Those who were disagree to give consent.
- Geriatric people were not willing to give interview.
- Seriously ill people.
- <60 year’s old people.
Study Area
The study was conducted in Agargaon and Savar old home and selected residential area.
Duration
The study completed within four months, April to October 2009.
Sampling Frame
All those elderly people who are staying with his/her family and old home considered as a sampling frame. The people aged ≥60 years are considered as a sampling unit.
Sample size calculation
The following formula will be used to calculation the sample size for our result
Formula
Here, U= error level, 1.28
V= significance level, 1.96
π = Proportion, 50%
π¸=Null hypothesis value, 30%
= 58
Cluster effect = 58 x 2.0 =116
n = 116+Drop out 10%
= 116+ (10 ÷100)
= 116.1
If we need 100, we have to take 110 samples
If we need 1 , we have to take110÷100 samples
If we need 116.1, we have to take (110÷100) x 116.1 samples
=127.71
So the total samples size is 127.71 or 128.
Randomization procedure:
The study shows that, the areas are in urban of Dhaka city. Two old homes and community were selected randomly from Agargaon and Savar. Then ≥60 year’s peoples were selected randomly from each group. List of the geriatric people were collected from old home’s registration number. Sample size was collected proportionally to each group.
List of Variables
a) Major Variables:
- Sex
- Occupation
- Education
- Monthly family income:
1. Assets benefit.
2. Other support: Land, Home, Money, Business.
- Health Care.
- Knowledge about nutrition.
- Knowledge about immunization.
b) Minor Variables:
- Age of geriatric people.
- Personal and environmental hygiene.
Data collection procedure:
Quantitative data collection:
Three types of quantities data were collected in the study.
A. Anthropometrics measurement (height, weight)
Weight was taken by US weighing machine. Height was taken using locally made height scale with a precision of 1 cm.
B. Data on food intake
24 hour recall method:
In 24 hour recalls method, their parents or caretakers were asked by nutritionist, who has been trained in interviewing techniques, to recall the subjects exact food intake during the previous 24 hour period or preceding day. Detailed descriptions of all foods and beverages consumed including cooking methods were recorded by the interviewer. Vitamin and mineral supplement used was also noted. Quantities of food consumed were usually estimated in household measures and entered on data sheet.
Data on food intake of the child was collected by 24-hour recall method by asking their presents.
C. Data on socio-economic status, childcare practices, food habit, personal hygiene:
Data on family income, childcare practices, food habit, personal and household hygiene and school’s environment were collected by structured questionnaire.
Data coding editing and entry:
As soon as the data are collected those were edited by the students coded rightly and was put on to entry by using suitable data entry software.
Data Analysis:
The study was visit various old-homes and took note about nutritional status, eating pattern, dietary intake and mental, physical status of elderly people. The study was followed descriptive method in this research.
The BMI defined as weight (kg) / (height) ² was used to assess the nutritional status of elderly people. According to WHO-
BMI M F
Standard 22.5 21.5
Over nutrition >25, Under nutrition <18
The studies used to analyze data by SPSS computer software.
The study found elderly people’s nutritional status of two groups. On top of that, the study came to know their BMI, support on that result it will able to know the level of malnutrition.
Quality control methods:
With due respect at first we would like to give thanks to our honorable teacher Dr. SK Roy, who helped us form the beginning to end of this research through his various activities and some of his reasonable, meaningful and valuable advices.
Data quality was controlled through tools verification (compare to standard tools) questionnaire, cross check editing, data entry, check and minimizing response errors through proven question.
It was the work of a great term where all the team members were very sincerer towards our research. We were very conscious for collecting any kinds of related information from any reliable source. Our team was very dedicated for research.
Literature review:
Limitation of the study:
The elderly or older people are the senior citizens of a country. They are very respectable in a family, community and in the state. The elderly population is increasing over the world. According to NIPORT, the statistics shows that 1.13 million people are above 60 years old, which is 7.1% of the total population. It is a matter of fact that in developing socio-economic condition elderly people not get much importance in regards to nutritional status and diet habit which is mandatory for healthy life.
The age structure of Bangladesh’s population is changing noticeably. Rapid fertility declines in the 1980s have decreased the proportion of young persons (1), and reductions in child mortality have increased life expectancy from 44 years in 1975 to 60 years in 2001. The population aged over 60 years currently represents about 7% of the 140 million population of Bangladesh (1) and is projected to represent 16% of the total population by 2050 (3). As the older population grows, the prevalence of chronic disease is also likely to grow. Understanding the burden of chronic disease in Bangladesh will guide the design of strategies to prevent chronic illness and provide health care to increasingly larger numbers of older people with chronic conditions.
In the United States, the recent geriatric certification examination jointly administrated by the American board of family practice and the American board of international medicine has caused controversy. The geriatric population represents a continuum of the family life cycle that already belongs within the reclaim to the family physician’s knowledge. The concern of discipline of geriatrics social supports, environmental assessment, occupational status, cognitive function, activities of daily living and physiological changes of organ- system are within the grasp of the practicing family physician. It is clear that majority of physicians who are in internal medicine or family practices are not knowledgeable about some aspects of geriatric medicine, because only 56% 0f 4282 examinees who sat the last examination were successful. Although a large minority failed, more than 90% of those who had some formal training are geriatric passed. These data indicate a need for family physicians to keep up data with the geriatric literature in light of expected increase of sub-population in our practices. The articles reviewed in this selection from current literature were chosen for their relevance based on the prevalence of the issues raised and applicability to any geriatric patient. It is seen that the knowledge and practice of geriatric nutrition is not in accepted level in USA even.
In view if the situation, we should follow the recommendation of WHO.
RDA Males:
| Nutrient | Males |
| Age | 55+ |
| Protein (gm) | 63 |
| Vitamin A (IU) | 5000 |
| Vitamin D (IU) | 200 |
| Vitamin E (IU) | 10 |
| Folic Acid (mcg) | 400 |
| Vitamin C (mg) | 60 |
| Calcium(mg) | 800 |
| Iron(mg) | 10 |
RDA Females:
| Nutrient | Females |
| Age | 55+ |
| Protein (gm) | 50 |
| Vitamin A (IU) | 4000 |
| Vitamin D (IU) | 200 |
| Vitamin E (IU) | 8 |
| Folic Acid (mcg) | 400 |
| Vitamin C (mg) | 60 |
| Calcium(mg) | 800 |
| Iron(mg) | 10 |
Limitation of the study:
Our group of two members conducted this study to assess the nutritional status of elderly people of Dhaka city. While conducting this study we had to overcome some obstacles.
1. Some person did not co-operate with us while collecting data using the questionnaires.
2. Different journals providing different information created confusions.
3. We had to face some problems as an unable ability books, journals, articles, research papers etc on our relevant topic.
4. Some person tried to hide some information about monthly income, dietary intake.
5. The study had to be limited to a small community due to shortage of time and resource.
6. Detailed history of dietary intake was collected through interviewers. But the investigators could not observe the quality & quantity of the food consumed.
Results
Discussion
RESULTS:
This cross sectional study was carried out among 127 male and female elderly people
1. GENERAL CHARACTERISTIC:
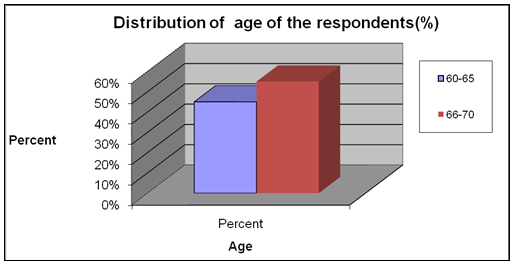
Figure: (Graphical presentation of Distribution of age of the respondents)
This graph show the distribution of aged majority between 66-70 aged 55%
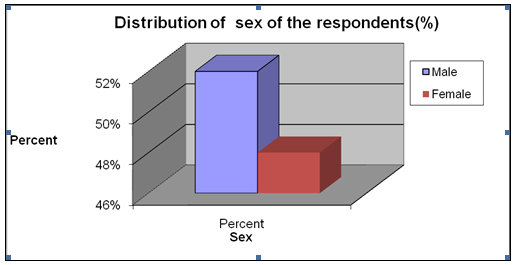
Figure: (Graphical presentation of Distribution of sex of the respondent)
This graph show the distribution of sex majority 52% are Male
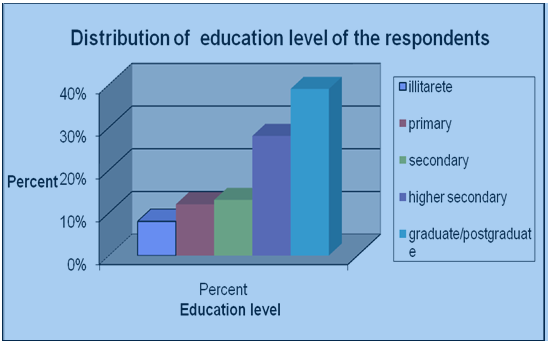
Figure: (Graphical presentation of Distribution of education level of the respondents)
This graph show the distribution of education level majority 39.40% were graduate / postgraduate
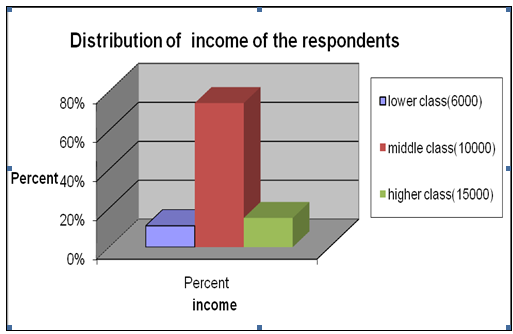
Figure: (Graphical presentation of Distribution of family status of the respondents)
This graph show the distribution of family status majority 74.0% were middle class
Source of the earning member of family of the respondents
Table
| Earning member | Number | Percent |
| Self | 45 | 35 |
| Husband | 30 | 23 |
| Son | 40 | 31 |
| Daughter | 10 | 8 |
| Others | 2 | 2 |
2.Health & Nutritional status
Distribution of height
Table
Height | Frequency | Parcent |
1.45-1.56 | 40 | 31.6 |
1.57-1.72 | 65 | 51.1 |
1.73-1.80 | 22 | 17.3 |
Total | 127 | 100 |
Distribution of Weight
Table
Weight | Frequency | Parcent |
40-64 | 64 | 52.7 |
65-70 | 57 | 42.5 |
79-90 | 06 | 04.8 |
Total | 127 | 100 |
Nutritional status of respondents by BMI
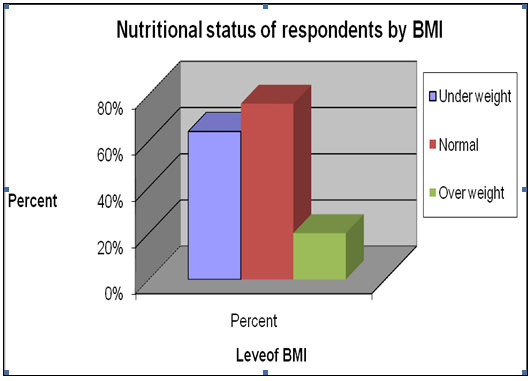
Figure: (Graphical presentation of Nutritional status of respndents by BMI)
This graph show the distribution of level of BMI majority 76% Normal
This graph show the food restriction on medical advice 56% were yes
This graph show the distribution of sleeping time 46.50% were good
This graph show the distribution of following checkup 55.10% were none
This graph show the distribution of taking medicine is 69 % were yes
3.FOOD PRACTICE THE RESPONDENTS
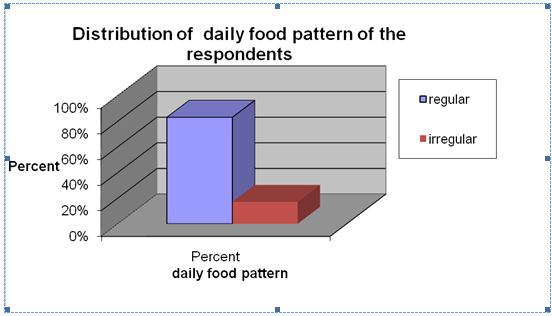
Figure: 1.16 (Graphical presentation of Distribution of daily food pattern of the respondents)
This graph show the distribution of majority 83% were regular
This graph show the distribution of fruit intake pattern 87% were naturally
This graph show the distribution of most of the people 61% were two time
This graph show the distribution of aged majority regularly walk were 76%
Distribution of type of treatment of the respondents
Table
Type of treatment | Number | percent |
| Specialized Doctor | 101 | 80 |
| Homeopathy | 20 | 15 |
| Ayurvadic | 3 | 2 |
| Others | 3 | 2 |
Table: 1.17 (The table shows the distribution of type of treatment of the respondents)
Distribution of food pattern of the respondents
Table
Food pattern | Number | percent |
| Fish, Meat | 110 | 87 |
| Egg, Meat | 14 | 11 |
| Vegetable, Pulse, Fruit | 3 | 2 |
Table: 1.17 (The table shows the distribution of food pattern of the respondents)
Pattern of water assumption by the respondents
Table
Water assumption | Number | percent |
| 1 Litre | 58 | 45 |
| 3 Litre | 44 | 34 |
| > 3 Litre | 25 | 19 |
Table: 1.17 (The table represents Pattern of water assumption by the respondents)
Protien intake of the respondents
Table
Protien (gm) | Number | percent |
7 | 4 | 3.1 |
8 | 15 | 11.8 |
9 | 11 | 8.7 |
10 | 39 | 30.7 |
11 | 29 | 22.8 |
12 | 23 | 18.1 |
13 | 2 | 1.6 |
14 | 4 | 3.1 |
Table: 1.17 (The table represents protein intake of the respondents)
Fat intake of the respondents
Table
Fat (gm) | Number | percent |
8 | 1 | 0.8 |
10 | 5 | 3.9 |
11 | 4 | 3.1 |
12 | 15 | 11.8 |
13 | 5 | 3.9 |
14 | 15 | 11.8 |
15 | 5 | 3.9 |
16 | 18 | 14.2 |
17 | 16 | 12.6 |
18 | 18 | 14.2 |
19 | 14 | 11 |
20 | 10 | 7.9 |
21 | 1 | 0.8 |
Table: 1.17 (The table represents fat intake of the respondents)
Total calorie intake by the respondents
Table
Calorie (Kcal) | Number | percent |
| 1400-1600 | 57 | 72 |
| 17-1900 | 64 | 18 |
| 2000-2100 | 6 | 8 |
Table: 1.17 (The table represents total calorie intake by the respondents)
DISCUSSION
We have worked on 127 elderly people of Dhaka city who belongs to middle class family. This was a descriptive study. We found many of the respondents were taking 30% less calorie. According to figure we saw that 55% people were between 66-70 years where 52% of them were male.Nearly 40% respondents were educated and 74% belongs to middle class family. 56% respondents were concious about the food restriction on medical advice. Almost 8S7% were having fruite intake natuarly. We found only 54% of the respondent drink bolied or purified water. After investigating the frequency of followup checking with doctor we found 55% of the respondents do not followup. We saw 46% of the respondents were having good sleep while 4% were unable to sleep. We found 61% respondents used to take food twice daily. Among the respondents 69% of them taking medicine regularly. 76% of the respondents used to walk in regular basis while 14% do not have the walking habit.
Recommendation:
15 | ||||||
| 14 | ||||||
| 13 | ||||||
| 12 | ||||||
| 11 | ||||||
| 10 | ||||||
| 9 | ||||||
| 8 | ||||||
| 7 | ||||||
6 | ||||||
| 5 | ||||||
| 4 | ||||||
| 3 | ||||||
| 2 | ||||||
| 1 | ||||||
WEEKS | PROTOCOL WRITING | DATA COLLECTION | DATA ENTRY | DATA ANALYSIS | THESIS WRITING | DISSEMINATION |
RECOMMENDATION
Keeping in mind the objective of this research we can recommend few steps to improve the nututional status of elderly people of Dhaka city. The recommendations are as follows:
- Care should be taken that the food must be balanced.
- Lead healthy life style including regular physical exercise.
- Aware people to drink safe and pure water.
- Regular medical checkup.
- Everyday fruiet and vegitable intake.
Conclusion:
Older age is a normal process of human’s life. Everyone get older at a particular time. They are senior citizens of a community, society and country. Bangladesh is a developing country. In our country geriatric people are not in good position. As families are becoming nuclear, people started to think these respected older people as the burden of their family. As result those old people get shelter in old homes. But it is not the actual picture; many of us love their parents and show responsibility to them.Elderly people are not only suffering of this problem, but also faces many health problem, such as paralysis problems from a stroke, parkinson’s disease, frail skins, dental carries, neurological problems, poverty, malabsorpation, peripheral vascular disease, osteo and rheumatoid arthritis, taste change, hearing problem and various chronic diseases.Under nutrition is becoming increasingly prevalent in the ever growing elderly population.
As can be seen, there is a complex web of factors affecting nutritional status in the elderly involving the ageing process itself, illness, drug treatment and socio-economic factors.Elderly are as risk if they are in an acute hospital, nursing or residential care on their own homes. We should care of them in every moment.
Deterioration of the nutritional status is associated with food consumption, recent weight loss, disease-associated stress, degree of self-sufficiency.
Hence it is necessary to pay special attention to functional capacity when planning nutritional care for this group, especially when they are debilitating by disease.
Sanitation is a major subject, what should be done properly. If their living places are unhealthy, various types of germs may attack them and cause various diseases. Most of them are underweight and they fulfill their food requirement mostly from carbohydrates. They are highly suffering from micronutrient deficiencies for their low intake of animal food and also nutrients. They have very poor knowledge about nutritive food. It is very necessary to create awareness among them.
They should be cared about their dietary intake, consumption of seasonal fruits, milk regularly. They should be careful about hygiene practices, sanitations and living place must be neat and clean, food must be balanced, drink safe water and wash hands before meal. As it is a very complicated part of life they should take doctor’s advice regularly.Though Government of Bangladesh has taken some steps for these elderly people which are not sufficient for good health of this target group. We should take care of these people. Moreover, our government should take some more effective measures to improve geriatric people’s health development. It is very much important to make bond among families and improve the nutritional status of elderly people.