A germ cell tumor (GCT) is a type of cancer that develops from germ cells, which are the cells that produce eggs in women and sperm in men. It is a neoplasm that develops from primordial germ cells. Germ-cell tumors can be cancerous or non-cancerous. Germ cells are normally found within the gonads (ovary and testis). GCTs that develop outside the gonads may be birth defects caused by embryo development errors.
Seminomatous and non-seminomatous germ cell tumors are the two main types. Seminomatous tumors have a better prognosis and respond better to radiation therapy, whereas non-seminomatous tumors are more aggressive and may necessitate a combination of treatments, including surgery, chemotherapy, and, in some cases, radiation therapy. These tumors can appear anywhere in the body, but they are most commonly found in the ovaries or testicles. They can, however, develop in other places, such as the mediastinum (the space between the lungs in the chest), the pineal gland in the brain, and other places.
Types
- Seminomatous: These tumors resemble early forms of germ cells and are more likely to be confined to the testes or ovaries. They are usually more responsive to treatment.
- Non-seminomatous: These tumors are more diverse and may contain different types of cells, such as embryonal carcinoma, yolk sac tumor, choriocarcinoma, and teratoma. They are often more aggressive and may require a combination of treatments.
Cause
Some researchers believe that this distribution results from abnormal migration of germ cells during embryogenesis. Others propose that germ cells are widely distributed to multiple sites during normal embryogenesis, with these cells conveying genetic information or performing regulatory functions at somatic sites.
Extragonadal GCTs were thought initially to be isolated metastases from an undetected primary tumor in a gonad, but many germ cell tumors are now known to be congenital and originate outside the gonads. The most notable is sacrococcygeal teratoma, which is the most common tumor diagnosed in newborns.
Diagnosis
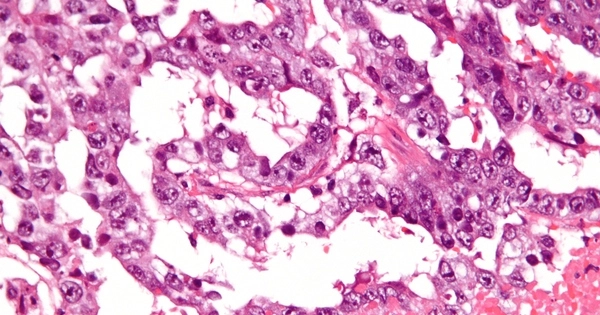
Diagnosis is typically made through a combination of imaging studies (ultrasound, CT scans, or MRI), blood tests (tumor markers), and biopsy. Treatment depends on the type and stage of the tumor. Surgery is often performed to remove the tumor, and additional treatments such as chemotherapy or radiation therapy may be used, especially for non-seminomatous tumors.
Treatment
Women with benign GCTs, such as mature teratomas (dermoid cysts), are treated with ovarian cystectomy or oophorectomy. In general, all patients with malignant GCTs undergo the same staging surgery as those with epithelial ovarian cancer. If the patient is in her reproductive years, a unilateral salpingoophorectomy with the uterus, ovary, and fallopian tube on the opposite side can be performed.
Patients with germ-cell cancer are frequently treated with combination chemotherapy for at least three cycles, but female patients with early-stage disease may not require this treatment. The chemotherapy regimen most commonly used in GCTs is known as PEB (or BEP), and it consists of bleomycin, etoposide, and a platinum-based antineoplastic (cisplatin). Targeted treatments, such as immunotherapy, hormonal therapy and kinase inhibitors, are being evaluated for tumors that do not respond to chemotherapy.