Dental caries is one of the most important chronic diseases affecting the children. It is also known as tooth decay or a cavity, is an infection, bacterial in origin, that causes demineralization and destruction of the hard tissues (enamel, dentin and cementum), usually by production of acid by bacterial fermentation of the food debris accumulated on the tooth surface. Among all the teeth of oral cavity, the first permanent molar is more vulnerable to caries because of its morphological & functional characteristics. There are four main criteria required for caries formation —Cariogenic Bacteria, Fermentable Carbohydrates, Susceptible Tooth Surface and Required Time.
There are 4 first permanent molars in the oral cavity of a human being. Some factors make this tooth the most vulnerable one for caries incidence. It is the first erupted permanent tooth of the oral cavity hence it remains the longest time in the mouth. On the other hand, its occlusal surface is a choice location of caries shortly after its emergence.
A person experiencing caries may not be aware of the disease. The earliest sign of a new carious lesion is the appearance of a chalky white spot on the surface of the tooth, indicating an area of demineralization of enamel. This is referred to as an incipient carious lesion or “micro cavity”. As the lesion continues to de-mineralize, it can turn brown but will eventually turn into a cavity. Before the cavity forms, the process is reversible, but once a cavity forms, the lost tooth structure cannot be regenerated. A lesion that appears brown and shiny suggests dental caries were once present but the demineralization process has stopped, leaving a stain. A brown spot that is dull in appearance is probably a sign of active caries.
As the enamel and dentin are destroyed, the cavity becomes more noticeable. The affected areas of the tooth change color and become soft to the touch. Once the decay passes through enamel, the dentinal tubules, which have passages to the nerve of the tooth, become exposed, resulting in a toothache. The pain may worsen with exposure to heat, cold, or sweet foods and drinks.
Dental caries can also cause bad breath and foul tastes. In highly progressed cases, infection can spread from the tooth to the surrounding soft tissues. Complications such as cavernous sinus thrombosis and Ludwig’s angina can be life-threatening.
The most effective brushing technique is Fone’s method. Fones’ method of tooth-brushing is the world recognized way of tooth-brushing, registered by World Health Organization (WHO) & American Dental Association (ADA). And, it is trustworthy among this particular population. The children, who are brushing during the night, are less vulnerable to caries. But, the ideal timing is “During Morning & Night”. It is not so much effective among the selected population. So, either the information given by the guardians is not absolutely correct or the children are using a wrong method of tooth-brushing.
Justification:
First permanent molars are the first erupting teeth of the oral cavity. It’s morphological & functional characteristics make this tooth the most vulnerable one. It remains the longest time in our mouth. So, it is easier for the cariogenic bacteria to cause caries in this tooth. Its occlusal surface is a choice location of caries, it is another important factor why this tooth may be affected & decayed.
First permanent molar plays a key role in maintaining the dental & overall health of an individual. It is the first tooth to erupt and exhibit a greater control over the teeth that erupt later behind and in front of it as they are forced to position to the already erupted & in occlusion functioning first molars. Moreover, they are the largest tooth in oral cavity and bear the maximum occlusal load. They are positioned in oral cavity in such a way that they influence the vertical distance of maxilla and mandible, the occlusal height and aesthetic proportions. Apart from this, since they have the maximum root surface area they are considered to be the best source of anchorage for moving the tooth. So, from various points, it is clear that the first permanent molar is the most important and key tooth of our oral cavity.
Children cannot maintain their oral hygiene status properly and most of the people of our country cannot get necessary dental treatment as it is considered as very expensive. As a result, the first permanent molar is extracted out of the mouth.
There is very limited research done regarding the caries status of the first permanent molar. So, this study would explore the present situation among the primary school going children and help to prevent the current circumstances by increasing awareness and taking different necessary steps.
Research question:
What is the status of dental caries in first permanent molars among the primary school going children?
Objectives:
General objectives:
To find out the status of dental caries in first permanent molars among the primary school going children.
Specific objectives:
- To determine the proportion of DMFT (Decayed Missed Filled Tooth) status among the primary school going children.
- To find out the oral hygiene practice of the study subjects.
- To find out the food habit of the study subjects.
- To find out the relationship of dental caries with age, gender, oral hygiene, food habit and occupation of the parents.
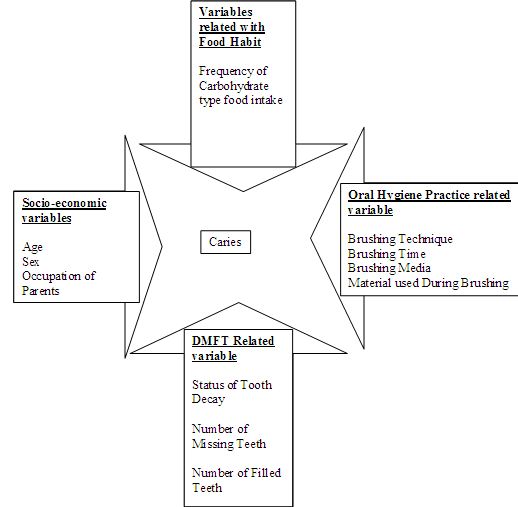
Conceptual Framework:
There are four main criteria required for caries formation —
1. Cariogenic Bacteria
2. Fermentable Carbohydrates
3. Susceptible Tooth Surface
4. Required Time
Variable list
Literature review:
Dental caries, also known as tooth decay or a cavity, is an infection, bacterial in origin, that causes demineralization and destruction of the hard tissues (enamel, dentin and cementum), usually by production of acid by bacterial fermentation of the food debris accumulated on the tooth surface. It usually occurs in children and young adults but can affect any person. It is a common cause of tooth loss in younger people.
Bacteria are normally present in the mouth. The bacteria convert all foods — especially sugar and starch — into acids. Bacteria, acid, food debris, and saliva combine in the mouth to form a sticky substance called plaque that adheres to the teeth. It is most prominent on the back molars, just above the gum line on all teeth, and at the edges of fillings. Plaque that is not removed from the teeth mineralizes into tartar. Plaque and tartar irritate the gums, resulting in gingivitis and ultimately periodontitis.
Plaque begins to build up on teeth within 20 minutes after eating (the time when most bacterial activity occurs). If this plaque is not removed thoroughly and routinely, tooth decay will not only begin, but flourish.
The acids in plaque dissolve the enamel surface of the tooth and create holes in the tooth (cavities). Cavities are usually painless until they grow very large and affect nerves or cause a tooth fracture. If left untreated, a tooth abscess can develop. Untreated tooth decay also destroys the internal structures of the tooth (pulp) and ultimately causes the loss of the tooth.
Enamel is a highly mineralized acellular tissue, and caries act upon it through a chemical process brought on by the acidic environment produced by bacteria. As the bacteria consume the sugar and use it for their own energy, they produce lactic acid. The effects of this process include the demineralization of crystals in the enamel, caused by acids, over time until the bacteria physically penetrate the dentin. Enamel rods, which are the basic unit of the enamel structure, run perpendicularly from the surface of the tooth to the dentin. Since demineralization of enamel by caries, in general, follows the direction of the enamel rods, the different triangular patterns between pit and fissure and smooth-surface caries develop in the enamel because the orientation of enamel rods are different in the two areas of the tooth.
As the enamel loses minerals, and dental caries progresses, the enamel develop several distinct zones, visible under a light microscope. From the deepest layer of the enamel to the enamel surface, the identified areas are the: translucent zone, dark zones, body of the lesion, and surface zone. The translucent zone is the first visible sign of caries and coincides with a one to two percent loss of minerals. A slight re-mineralization of enamel occurs in the dark zone, which serves as an example of how the development of dental caries is an active process with alternating changes. The area of greatest demineralization and destruction is in the body of the lesion itself. The surface zone remains relatively mineralized and is present until the loss of tooth structure results in cavitations.
Degree of caries is detected by DMFT (Decayed Missed Filled Tooth) status. DMFT describes the amount and prevalence of dental caries in an individual. DMFT means to express the caries prevalence numerically and are obtained by calculating the number of Decayed (D), Missing (M), Filled (F) and Teeth (T).
It is thus used to get an estimation illustrating how much the dentition until the day of examination has become affected by dental caries. It is calculated for 28 (permanent) teeth.
How many teeth have caries lesions?
How many teeth have been extracted?
How many teeth have fillings or crowns?
The sum of the three figures forms the DMFT value. For example: DMFT of (4 + 3 + 9) = 16 means that 4 teeth are decayed, 3 teeth are missing and 9 teeth have fillings. It also means that 12 teeth are intact.
Dental caries is one of the most common diseases of the oral cavity in our country. Most of the people are unaware about the maintenance of oral hygiene practice. Specially, the children cannot clean their teeth and mouth properly. As many people are unaware about the take care of their own teeth; many complicated diseases (periapical abscess, radicular cyst) etc. Besides, when pain is initiated by caries; that sort of pain is very much acute, intensive and radiating in nature.
Some studies have been taken place in Bangladesh. The DMFT statuses of this study indicate that the caries indexes of our countrymen are pretty much high.
A study in 1990 stated that; the DMFT score of the urban privileged children was 5.0; whether the mean DMFT-values ranged from 1.1 (urban privileged 6 year olds) to 4.7 (rural 34-45 year olds). The percentage of 12 year old children affected by caries was higher than in the 18 and 35-45 year olds in all socioeconomic groups.
A descriptive study emphasized upon the oral health of 12 year old Bangladeshi children. They found out that; though the DMFT score was comparatively low (0.97), poor oral hygiene was frequently detected among the subjects.
The DMFT status of the first permanent molars among the primary school going children of Saudi Arabia was 2.74. The caries prevalence in first permanent molar was significantly high as age increased.
Valuable information can be obtained from different Middle Eastern & Central European journals that the caries index of the first permanent molars are pretty high among the primary school going children.
To obtain the caries experience and, plaque accumulation severity and pit and fissure morphology in first permanent molars in 7-8 children in Wuhan, as a reasonable prediction of caries risk and preventive attention in the future, a convenient sample of five primary schools in the vicinity of the Wuhan University School and Hospital of Stomatology was drawn. Two calibrated examiners orally examined all present grade 2 children in the classroom, using standard caries plaque and tooth morphology criteria. Dental caries was scored at enamel (D(2)) and dentine (D(3)) for tooth and surface level. Independent variables were age, gender and school. Data analysis used analysis of variance and t-test. The sample comprised 1 043 7- and 8-year-olds. The prevalence of dental caries in permanent dentition was 8.7% and in primary dentition, 68.7%. Mean Decayed, Missing, Filled Teeth/S (DMFT/S) scores were 0.11 and 0.14, respectively. Mean dmft/s scores were 2.8 and 5.0. The d-component constituted 75% of the d(3)mft index, while enamel carious lesions constituted 36% of the total number of carious lesions (d(2,3)-component). Prevalence of medium and deep pits and fissures was 84.6%. Prevalence of medium and severe plaque accumulation was 67.4%. Prevalence of dental caries in the deciduous and permanent dentitions of 7- to 8-year-old children was high. Deep pits and fissures in high caries risk children should be sealed.
To survey the tooth decay of the first molars among the people in area of northeast China in order to provide the foundation for prevention and treatment strategies of caries. According to the third national oral health investigation of epidemiology, the dental caries of first permanent molars were examined among 9394 people aged 5, 12, 35-44 and 65-74 in northeast China. The data were analyzed by SPSS 13.0 statistical software. Dental caries prevalence rate and DMFT (dmft) of first permanent molar were calculated.
The prevalence of crown and root dental caries in northeast China were 26.86% and 3.81% respectively, mean DMFT (dmft) of crown and root dental caries were 0.41 and 0.04 respectively. There were significant differences of dental caries among provinces in northeast China. Mandibular first molar suffered from dental caries easily. The prevalence of caries of female was higher than that of male (P<0.01), but there was no significant difference of prevalence of root caries between two sexes (P>0.05). Except Jilin province, there were significant differences of prevalence of crown caries between city and rural area in Liaoning and Heilongjiang provinces (P<0.01). It was no significant difference of prevalence and mean DMFT (dmft) of root caries between city and rural area in each province (P>0.05).
The prevalence of dental caries of the first molar among the people in northeast China is high. The dental caries prevention and cure of first permanent molar should be emphasized in oral health field.
To study the prevalence of dental caries in primary dentition of 5-year-old children in Northeast of China, and assess the risk factors for dental caries.
The representative samples were selected by multi-stage, stratified and random sampling from the three provinces of Northeast of China. Dental caries of 2353 children at five-year age were recorded according to WHO criteria. The questionnaire were finished by 1191 parents of the children and analyzed with X(2) test and logistic regression using SPSS 12.0 software package.
The prevalence of dental caries in 5-year-old children was 75.82% and dmft was 4.63. The lowest caries prevalence was noted in Heilongjiang province. The important predictors of dental caries were the educational level of parents (P<0.001) and eating sweet food before sleep (P=0.006).
To reduce the dental caries in primary dentition, oral health education for the parents should be emphasized and sugar-intake before sleeping should be controlled.
Dental caries is one of the most prevalent chronic diseases in children and DMFT index is the most important quantitative factor for measuring tooth health. The purpose of the present study was to determine prevalence and bilateral occurrence of first permanent molar caries in 12-year-old Iranian students.
This cross-sectional study was carried out on 563 twelve-year-old students (307 boys and 256 girls), randomly selected from private and public schools. All students were examined clinically for dental caries using the World Health Organization (WHO) criteria by a specialist on a dental chair in Rafsanjan Dental School. Data was analyzed using chi-square and t-test.
The mean DMFT score of first permanent molars was 1.9 ± 1.6 (1.83 boys, 1.98 girls) and 31.4% (32.9% boys, 29.7% girls) of the students were caries free. There were no significant differences between boys and girls. Decayed (D) component yielded to be 40.9%, missing (M) 0.35% and filled (F) 6.22%. Maxillary and mandibular first permanent molars had 80.8% and 84% bilateral caries occurrence, respectively. There were no significant differences between the caries prevalence of right and left sides.
Caries prevalence among 12-year-old students in Rafsanjan, Iran is less than the global standards of WHO and FDI for 2000, but close to the gold standard for 2010. Bilateral caries occurrence in the first permanent molars was concluded to be high in the study population.
The carious status of the first permanent molar (FPM) was studied in 432 school children (aged 9–12 years) from a randomly selected primary schools from Sharfia area of Jeddah, Kingdom of Saudi Arabia. The sample consisted of 108 children from each age group of 9, 10, 11, and 12 years old. In total, 24.5% had all of their FPMs sound and 6% had all FPMs carious. The prevalence of four sound FPMs varied according to age with the highest (33%) amongst the nine-year olds and the lowest (16.5%) in the oldest children (12 years). Almost one-third (32.5%) of the children, who knew the age of eruption of the FPMs, had all of their molars sound. The children who had received advice regarding oral hygiene from a dentist or parent had more sound FPMs compared to the children who did not receive any advice. The number of carious FPMs increased with age. The prevalence of caries of the FPM was high and increased with increasing age. The level of knowledge had a positive correlation with the caries levels amongst this cohort of scholars.
Methodology:
Design of the study:
The study was analytical type of cross-sectional study.
Study Area:
Study was conducted in Wide Vision School, Uttara in Dhaka city.
Study period:
This study was conducted for 4 months (Jan-April 2013).
Study population:
Primary school children, aged from 6 years to 13 years.
Selection of participants:
Inclusion Criteria:
The following populations were included from the study
a. Primary school children
b. Are aged from 6-13 years
c. Suffering from dental caries
Exclusion Criteria:
The following populations were excluded from the study
a. Uncooperative subject
b. Guardian not interested to the study
c. Handicapped subject
Data collection instruments:
- Pre-tested structured questionnaire
- Observation list
Data collection tools:
Dental instruments including
- Caries probe
- Dental mirror
- Disinfectants
Sampling Method:
All those children living in Uttara suburb and going to primary schools are considered as sampling frame. And the children of age 6-12 years of age and having caries in first permanent molars are considered as sampling unit. The sampling method was purposive.
Therefore, the estimated sample size is 384, but owing to the limitations of data (scarcity of fund and time etc); the sample size was restricted to 266.
Quality of data:
Data were collected by the researcher himself. After collection of data, missing values were identified for consistency and accuracy.
Data analysis plan:
The data were analyzed by using SPSS-16. Descriptive statistics were used for analysis.
Ethical consideration:
All ethical issues related to research are addressed according to the guidelines of research ethical review committee of the American International University.
i) Permission from American International University, Bangladesh was obtained as pre-requisite.
ii) Informed consent by using form translated into local language “Bangla” were taken before the interview and clinical examination.
iii) Respondents have the right to refuse and withdraw from the study at any time.
iv) Confidentiality of respondents is strictly maintained.
Results:
The results of the study findings are presented here in Tables and graphs with interpretations
Table: The Characteristics of the Study Subjects (n=266)
| Variables | Frequency (n) | Percentage (%) |
| Age | ||
| 6-9 years | 138 | 52.0% |
| 10-13 years | 128 | 48.0% |
| Mean±SD (years) | 9.6±2.1 | |
| Gender | ||
| Male | 131 | 49.0% |
| Female | 135 | 51.0% |
| Occupation of the child’s father | ||
| Business | 143 | 54.0% |
| Service holder | 123 | 46.0% |
| Occupation of the child’s mother | ||
| Housewife | 234 | 88.0% |
| Service holder | 32 | 12.0% |
Table-1 shows that the age & gender of the primary school going children and occupation of their parents. Fiftytwo percent of the subjects are under age group 6-9 years and 48% are under age group 10-13 years. Where 49% of them are male and 51% are female. Fiftyfour percent of the child’s fathers are businessman and 46% are service holder. And 88% of child’s mothers are house wife and 12% are service holder.
Table : The Food Habit of the Respondents in a Usual Week (n=266)
| Variables | Frequency (n) | Percentage (%) |
| Having Burger and Sandwich in a usual week | ||
| Do not take | 138 | 51.9% |
| Rarely take | 109 | 41.0% |
| Almost everyday | 13 | 4.8% |
| Daily | 6 | 2.3% |
| Having Chocolate and Chewing gum in a usual week | ||
| Do not take | 62 | 23.3% |
| Rarely take | 130 | 48.9% |
| Almost everyday | 38 | 14.3% |
| Daily | 36 | 13.5% |
| Having of ice cream in a usual week | ||
| Do not take | 144 | 54.1% |
| Rarely take | 89 | 33.5% |
| Almost everyday | 27 | 10.2% |
| Daily | 6 | 2.3% |
| Having of cold drinks in a usual week | ||
| Do not take | 135 | 50.8% |
| Rarely take | 96 | 36.1% |
| Almost everyday | 20 | 7.5% |
| Daily | 15 | 5.6% |
Table-2 shows that the food habits of the respondents in a usual week. It shows that 51.9% of subjects don’t take burger and sandwich in a usual week. 41% of them rarely take burger and sandwich in a usual week. Simultaneously 4.8% and 2.3% take burger and sandwich in a usual week almost every day and daily. About twenty three of the subjects don’t take chocolate & chewing gum in a usual week. 48.9% of them rarely take chocolate & chewing gum in a usual week. Simultaneously 14.3% and 13.5% take chocolate & chewing gum in a usual week almost every day and daily. About fiftyfour percent of the subjects don’t take ice-cream in a usual week. 33.5% of them rarely take ice-cream in a usual week. Simultaneously 10.2% and 2.3% take ice-cream in a usual week almost every day and daily. About fiftyone percent of the subjects don’t take cold drinks in a usual week. 36.1% of them rarely take cold drinks in a usual week. Simultaneously 7.5% and 5.6% take cold drinks in a usual week almost every day and daily.
Table: The Practice of Tooth Brushing of the Respondents (n=266)
| Variables | Frequency (n) | Percentage (%) |
| The timing of brushing teeth in a usual day | ||
| Follow the recommended timing (at least morning and night) | 113 | 42.5% |
| Do not follow | 153 | 57.5% |
| Brushing technique | ||
| Fone’s (Properly) | 42 | 15.8% |
| Not properly | 123 | 46.2% |
| Other ways | 101 | 28.0% |
| Use of toothpaste | ||
| Pepsodent | 78 | 29.3% |
| Colgate | 78 | 29.3% |
| Close up | 45 | 16.9% |
| Meswak | 10 | 3.8% |
| Sensodyne | 8 | 3.0% |
| Unable to mention | 15 | 5.6% |
| Others | 24 | 9.0% |
Table-3 shows the practice of tooth brushing of the respondents. It shows that 42.5% of the respondents brush their teeth as recommended by the dentists (twice daily) and 57.5% do not follow the trend. About sixteen percent of the respondents follow the Fone’s technique of teeth brushing. Where 46.2% don’t brush properly and 28% follow other ways. Use of tooth paste by the respondents are as follows Pepsodent (29.3%), Colgate (29.3%), Close up (16.9%), Meswak (3.8%), Sensodyne (3.0%), Unable to mention (5.6%), Others (9.0%).
Table : The Distribution of the Respondents by Status of the Missed and Filled Teeth
| Variables | Frequency (n) | Percentage (%) |
| Missed teeth | ||
| No tooth missing | 183 | 68.8% |
| Permanent first molar | 3 | 1.1% |
| Other permanent teeth | 11 | 4.1% |
| Deciduous teeth | 69 | 25.9% |
| Filled teeth | ||
| No tooth filled | 246 | 92.5% |
| Permanent first molar | 4 | 1.5% |
| Other permanent teeth | 2 | 0.8% |
| Deciduous teeth | 14 | 5.3% |
Table-4 shows the distribution of the respondents by status of the missed and filled teeth. The table shows that 68.8% of the respondents have no tooth missing. 1.1% has permanent first molar missing, 4.1% has other permanent teeth missing & 25.9% has missing deciduous teeth. About ninetytwo percent of the respondents have no tooth filled. 1.5% has permanent first molar filled, 0.8% has other permanent teeth filled & 5.3% has deciduous teeth filled.
Table : The Relationship of the Dental Caries with the Variable of Interest
| Variables | Status of the dental caries | Chi-square (χ2) value | p-value | |
| Age | Yes | No | ||
| 6-9 yrs | 95 (58.6%) | 43 (41.3%) | 7.590 | 0.006 |
| 10-13 yrs | 67 (41.4%) | 61 (58.7%) | ||
| Sex | ||||
| Male | 49 (47.1%) | 82 (50.6%) | 0.311 | 0.577 |
| Female | 55 (52.9%) | 80 (49.4%) | ||
| Occupation of the father | ||||
| Business | 86 (53.1%) | 57 (54.8%) | 0.075 | 0.802 |
| Service holder | 76 (46.9%) | 47 (45.2%) | ||
| Occupation of the mother | ||||
| Housewife | 145 (89.5%) | 89 (85.6%) | 0.924 | 0.336 |
| Service holder | 17 (10.5%) | 15 (14.4%) | ||
| The timing of brushing teeth | ||||
| Do not follow ideal timing | 74 (45.7%) | 39 (37.5%) | 1.734 | 0.188 |
| Follow ideal timing | 88 (54.3%) | 65 (62.5%) | ||
| The learning source of brushing technique | ||||
| Family members | 141 (87.0%) | 92 (88.5%) | 0.691 | 0.708 |
| Dentist | 6 (3.7%) | 2 (1.9%) | ||
| Self learning | 15 (9.3%) | 10 (9.6%) | ||
| Brushing technique | ||||
| Fone’s (properly) | 26 (16.0%) | 16 (15.4%) | 4.080 | 0.130 |
| Not properly | 82 (50.6%) | 41 (39.4%) | ||
| Other ways | 54 (33.3%) | 47 (45.2%) | ||
| Having Burger and Sandwich in a usual week | ||||
| Do not take | 85 (52.5%) | 53 (51.0%) | 6.398 | 0.035 |
| Rarely take | 61 (37.7%) | 48 (46.2%) | ||
| Almost everyday | 10 (6.2%) | 3 (2.9%) | ||
| Daily | 6 (3.7%) | 0 (0.0%) | ||
| Having Chocolate and Chewing gum in a usual week | ||||
| Do not take | 36 (22.2%) | 26 (25.0%) | 2.302 | 0.512 |
| Rarely take | 77 (47.5%) | 53 (51.0%) | ||
| Almost everyday | 23 (14.2%) | 15 (14.4%) | ||
| Daily | 26 (16.0%) | 10 (9.6%) | ||
| Having Ice cream in a usual week | ||||
| Do not take | 77 (47.5%) | 67 (64.4%) | 7.570 | 0.026 |
| Rarely take | 61 (37.7%) | 28 (26.9%) | ||
| Almost everyday | 20 (12.3%) | 7 (6.7%) | ||
| Daily | 4 (2.5%) | 2 (1.9%) | ||
| Having Cold drinks in a usual week | ||||
| Do not take | 81 (50.0%) | 54 (51.9%) | 1.235 | 0.723 |
| Rarely take | 59 (36.4%) | 37 (35.6%) | ||
| Almost everyday | 11 (6.8%) | 9 (8.7%) | ||
| Daily | 11 (6.8%) | 4 (3.8%) | ||
Table-5 shows the relationship of the dental caries with the variable of interest. The variables are age, sex, occupation of father, occupation of mother, timing of brushing teeth, learning source of brushing technique, having burger and sandwich in a usual week, having chocolate and chewing gum in a usual week, having ice-cream in a usual week and having cold drinks in a usual week.
In case of age, in the 6-9 years age group 95 (58.6%) respondent has dental caries and in the 10-13 years age group 67 (41.4%) respondent has dental caries. Here the p-value (0.006) is significant.
In male 49 (47.1%) and in female 55 (52.9%) respondent has dental caries. Here the p-value (0.577) is not significant.
In case of occupation of father, 86 (53.1%) child whose fathers are businessman has dental caries and 76 (46.9%) child whose fathers are service holder has dental caries. Here the p-value (0.802) is not significant.
In case of occupation of mother, 145 (89.5%) child whose mothers are housewife has dental caries and 17 (10.5%) child whose mothers are service holder has dental caries. Here the p-value (0.336) is not significant.
In case of timing of brushing teeth, 74 (45.7%) respondent who do not follow ideal timing has dental caries and 88 (54.3%) respondent who follow ideal timing has dental caries. Here the p-value (0.188) is not significant.
In case of learning source of brushing technique, 141 (87%) respondent who learnt from family, 6 (3.7%) respondent who learnt from a dentist and 15 (9.3%) respondent who learnt by their own has dental caries. Here the p-value (0.708) is not significant.
In case of brushing technique, 26 (16%) respondent who brush teeth ideally, 82 (50.6%) respondent who do not brush teeth properly and 54 (33.3%) who follows other ways of brushing technique has dental caries. Here the p-value (0.130) is not significant.
In case of frequency of having burger and sandwich in a usual week, 85 (52.5%) respondent who do not eat, 61 (37.7%) respondent who rarely eat, 10 (6.2%) respondent who eat almost every day and 6 (3.7%) respondent who eat daily has dental caries. Here the p-value (0.035) is significant.
In case of frequency of having chocolate and chewing gum in a usual week, 36 (22.2%) respondent who do not take, 77 (47.5%) respondent who rarely take, 23 (14.2%) respondent who take almost every day and 26 (16%) respondent who take daily has dental caries. Here the p-value (0.512) is not significant.
In case of frequency of having ice-cream in a usual week, 77 (47.5%) respondent who do not take, 61 (37.7%) respondent who rarely take, 20 (12.3%) respondent who take almost every day and 4 (2.5%) respondent who take daily has dental caries. Here the p-value (0.026) is significant.
In case of frequency of having cold drinks in a usual week, 81 (50%) respondent who do not take, 59 (36.4%) respondent who rarely take, 11 (6.8%) respondent who take almost every day and 11 (6.8%) respondent who take daily has dental caries. Here the p-value (0.723) is not significant.
Discussion:
Male and female caries index ratio is almost equal. Here, sound teeth of male are 49 percent and female are 55 percent. The percentage of affected teeth ratio is approximately 1: 1.
Among all the selected populations, 1/4th of children are affected from First Permanent Molar caries. Here, the percentage of first permanent molar caries rate is 24.4%.On the other hand, almost half of the population are affected from deciduous molar caries. About one – third of the children are suffering from dental caries in more than three teeth. So, a large number of children are not able to maintain their oral hygiene properly.
It is seen that age of the respondents is an important factor for the occurrence of dental caries. The whole population is divided into two separate age groups. (6 – 9) & (10 – 13) years of age. Here, it is pointed that, the junior group (6 – 9) are more affected from dental caries rather than the other group (10 – 13).
With increase of age the rate of dental caries decreases. Where the p-value is 0.006, which is significant. It means the lower age group could not maintain their oral hygiene properly.
The percentage of the respondents having at least one tooth decayed is very high. Around three-fifth of the respondents has decayed tooth.
As the age increases, the rate of missing permanent teeth in the oral cavity escalates. On the other hand, the missing rate of the deciduous teeth is pretty high among the (6 – 9) years of age group.
Operative type of dentistry (filling) is done more in the deciduous teeth of the (6 – 9) years of age.
The occupations of the parents do not have any significant effect on the dental caries. Whether the father is businessman or service holder the p-value (0.802) is not significant and the mother is house wife or service holder the p-value (0.336) is not significant. Thus it is important for both of the parents who are working or not, help their child to maintain their oral hygiene.
The timing of brushing teeth, learning source of brushing technique and brushing technique followed by the respondents do not have significant effect on dental caries according to the study. However a large percentage of respondent are affected with dental caries either they are following the ideal timing (around half of the affected) or not. Almost same is seen in the case of learning source of brushing technique and brushing technique followed by the respondents.
The children, who are brushing during the night, are less vulnerable to caries. But, the ideal timing is “During Morning & Night”. It is not so much effective among the selected population. So, either the information given by the guardians is not absolutely correct or the children are using a wrong method of tooth-brushing.
The eating habits of the respondents have a great effect on dental caries. Frequent burger, sandwich and ice-cream intake have great significance on the dental caries. The p-value for frequency of having burger and sandwich in a usual week is 0.035, which is significant. And the p-value for frequency of having ice-cream in a usual week is 0.025, which is also significant.
Chocolate and chewing gum / cold drinks are also cariogenic foods. But, they are not as cariogenic as burger and sandwich / ice-cream.
Conclusions:
The following conclusions are drawn in relation to present study findings:
Male and Female decayed teeth status are almost same. Burger / sandwich and ice-cream are the most caries causing food than the others. Total population is divided into two different groups: 6 – 9 years of age and 10 – 13 years of age. Between the two groups, the first one is more vulnerable to caries. While the age increases, the missing rate of permanent teeth gradually increases. On the other hand, it is just opposite about the deciduous teeth. Operative type of dentistry (filling) is done more in the deciduous teeth of the (6 – 9) years of age. The children who are brushing during the night are less vulnerable to caries. But, the ideal timing is “During Morning & Night”. It is not so much effective among the selected population. So, either the information given by the guardians is not absolutely correct or the children are using a wrong method of tooth-brushing.
Limitations
- Due to time and resource constraints only 266 data were collected.
- The study was limited in a selected urban area of Bangladesh, therefore the result cannot be generalized to all over the country.
Recommendations
1. Children are extremely fond of Ice-cream / burger and sandwich / chocolate and chewing gum/ cold drinks. So, after taking such foods, the parents must wipe out the food particles from the tooth surfaces by tooth-brushing. Parents should be informed about this phenomenon.
2. Extra pre-caution should be taken for the children of (6 – 9) years of ages.
3. Brushing technique & time is the most important factor for proper tooth-brushing. Proper brushing technique is enough for caries prevention.
4. Brushing must be done two times a day. Not more than or not less than that. If, any person wants to do it single time in a day – it should be done at night before going to sleep.
5. Country wise awareness should be performed among the parents, guardians & teachers.
6. Caries prevention methods, proper brushing technique & list of carious foods can be added in the text books. School teacher counseling may be a good option.
7. Another way is the utilization of mass media (televisions / radio / advertisements etc).
8. This study has been conducted with limited time and resource therefore highly recommended for further study.
















