Choriocarcinoma is a type of cancer that develops in the tissues of the placenta, the organ that develops during pregnancy to nourish the fetus. It is a trophoblastic cancer that usually affects the placenta. This rare and aggressive cancer develops from trophoblast cells, which are responsible for the formation of the placenta.
It is distinguished by early hematogenous spread to the lungs. It is at the malignant end of the spectrum in gestational trophoblastic disease (GTD). It is also known as a germ cell tumor and can develop in the testis or ovaries.
Cause
Choriocarcinoma can be either gestational (related to pregnancy) or non-gestational. Gestational choriocarcinoma is most commonly associated with a molar pregnancy, a rare condition in which abnormal tissue grows in the uterus after conception. Non-gestational choriocarcinoma can develop in organs other than the uterus, such as the ovaries or testes.
Signs and symptoms
Common symptoms of choriocarcinoma include abnormal vaginal bleeding, a rapidly enlarging uterus, and elevated levels of beta-human chorionic gonadotropin (β-hCG), a hormone produced during pregnancy. The cancer has a tendency to spread quickly to other parts of the body, including the lungs, liver, and brain.
- increased quantitative chorionic gonadotropin (the “pregnancy hormone”) levels
- vaginal bleeding
- shortness of breath
- hemoptysis (coughing up blood)
- chest pain
- chest X-ray shows multiple infiltrates of various shapes in both lungs
- can present with decreased thyroid-stimulating hormone (TSH) due to hyperthyroidism.
Pathology
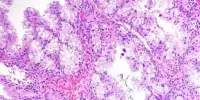
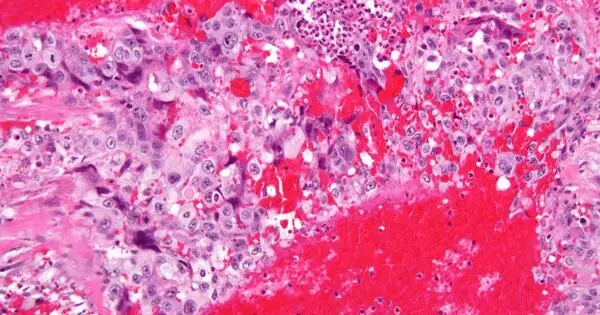
The identification of closely related syncytiotrophoblasts and cytotrophoblasts without the formation of distinct placental type villi is a distinguishing feature. Because choriocarcinomas contain syncytiotrophoblasts (beta-human chorionic gonadotropin-producing cells), they cause elevated blood levels of beta-human chorionic gonadotropin.
Syncytiotrophoblasts are multinucleated, multicellular cells with eosinophilic cytoplasm. They frequently encircle the cytotrophoblasts, resembling their normal anatomical relationship in chorionic villi. Cytotrophoblasts are polyhedral, mononuclear cells with hyperchromatic nuclei and cytoplasm that is clear or pale. Extensive hemorrhage is a common occurrence.
Treatment
Treatment for choriocarcinoma often involves a combination of chemotherapy and, in some cases, surgery. The choice of treatment depends on factors such as the extent of the disease, the patient’s overall health, and whether the cancer is gestational or non-gestational.
Because gestational choriocarcinoma (which develops from a hydatidiform mole) contains paternal DNA (and thus paternal antigens), chemotherapy is extremely effective. When using chemotherapy for invasive mole and choriocarcinoma, the cure rate is more than 90%, even for metastatic gestational choriocarcinoma.
As of 2019, single-agent methotrexate or actinomycin-D treatment is recommended for low-risk disease, while EMACO (etoposide, methotrexate, actinomycin D, cyclophosphamide, and vincristine (Oncovin)) treatment is recommended for intermediate or high-risk disease.