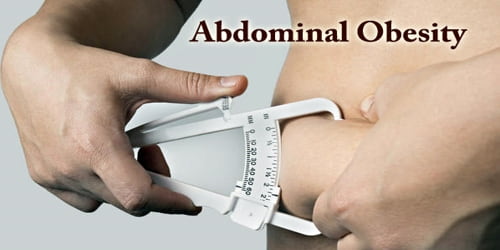
Abdominal Obesity
Definition: Abdominal Obesity (or “central adiposity”) occurs when excessive abdominal fat around the stomach and abdomen has built up to the extent that it is likely to have a negative impact on health. The terms sound very complicated, but they are simply different ways of describing belly fat. If people carry too much fat around their belly, they have abdominal obesity.
Excess body fat contributes to the major causes of death and disability, including heart attacks, strokes, high blood pressure, cancer, diabetes, osteoarthritis, fatty liver, and depression. Abdominal obesity is not confined only to the elderly and obese subjects. Abdominal obesity has been linked to Alzheimer’s disease as well as other metabolic and vascular diseases.
Moreover, people have only recently begun to understand the important endocrine and paracrine functions of intra-abdominal adipocytes, and the complex interactions leading to a diabetogenic and atherogenic metabolic risk profile.
Abdominal obesity was more closely related to metabolic dysfunctions connected with cardiovascular disease than was general obesity.
How to Measure: There are different ways to measure and assess belly fat. Abdominal obesity can be measured at the doctor’s office. The physician may use expensive scanning equipment to see exactly where fat is located in people’s belly. But those tests can be costly and may be inconvenient.
There are easier ways to measure abdominal obesity. Each method requires a flexible tape measure (like the ones used for sewing) and takes just minutes to perform.

Health risks: Abdominal obesity is associated with a statistically higher risk of heart disease, hypertension, insulin resistance, and Diabetes Mellitus Type 2. With an increase in the waist to hip ratio and overall waist circumference the risk of death increases as well. Metabolic syndrome is associated with abdominal obesity, blood lipid disorders, inflammation, insulin resistance, full-blown diabetes, and increased risk of developing cardiovascular disease. It is now generally believed that intra-abdominal fat is the depot that conveys the biggest health risk.
Although the health hazards of obesity are well established, obese individuals are not all at equal risk of developing a disease, which reflects the heterogeneity of this condition. The regional distribution of body fat is now recognized as a very important component of obesity-related health hazards. It is now generally accepted that the fat located within the abdominal cavity, the visceral fat, is the best correlate of most of the highly atherogenic metabolic complications seen in individuals with abdominal obesity.
People with obesity are also more likely to be hospitalized for asthma. A study has stated that 75% of patients treated for asthma in the emergency room were either overweight or obese. Alzheimer’s disease and abdominal obesity have a strong correlation and with metabolic factors added in, the risk of developing Alzheimer’s disease was even higher. Based on logistic regression analyses, it was found that obesity was associated with an almost 10-fold increase risk of Alzheimer’s disease.
Development of Abdominal obesity: The prognostic importance of high waist circumference has been recognized within the diagnostic criteria to identify individuals with features of the metabolic syndrome.
There are various ways of measuring abdominal obesity including:
- Absolute waist circumference (>102 cm (40 in) in men and >88 cm (35 in) in women)
- Waist-hip ratio (the circumference of the waist divided by that of the hips of >0.9 for men and >0.85 for women)
- Waist-to-height ratio
- Sagittal Abdominal Diameter
Typically, upper body obesity (android, ‘apple shape’ obesity) is more commonly found in men, whereas lower body obesity (gynoid, ‘pear shape’) is more commonly found in women.
In the USA National Health and Nutrition Examination Survey (NHANES) cohort examined between 1988 and 1994, 30% of men and 46% of women were abdominally obese, 16 according to the arbitrary waist circumference cut-offs of >102 cm in men and of >88 cm in women proposed by the National Cholesterol Education Program-Adult Treatment Panel III (NCEP-ATP III).17 By 1999–2000, these figures had risen to 36 and 52%, respectively.
Abdominal obesity (or Central obesity) is positively associated with coronary heart disease risk in women and men. It has been hypothesized that the sex differences in fat distribution may explain the sex difference in coronary heart disease risk.
A permanent routine of exercise, eating healthily, and, during periods of being overweight, consuming the same number or fewer calories than used will prevent and help fight obesity.
Information Source: